primary sclerosing cholangitis (PSC)



















Primary sclerosing cholangitis (PSC) is an uncommon inflammatory condition, which affects the biliary tree resulting in multiple strictures, liver damage, and eventually cirrhosis.
The diagnosis can be made when there are classical imaging features in the correct clinical context, and secondary causes of cholangitis have been excluded .
Epidemiology
PSC is strongly associated with inflammatory bowel disease (IBD) (in 70% cases ), especially ulcerative colitis, and thus shares similar demographics: young to middle-aged males (~4 decade) are most frequently affected .
Clinical presentation
The average age of diagnosis is 54 years (range 6-93) with increased occurrence in men (63%) . A large number of asymptomatic individuals are identified upon investigation of persistently deranged liver function tests. Symptomatic individuals commonly present non-specifically with fatigue. More specific symptoms include pruritus, jaundice or GI bleeding .
Pathology
Unfortunately, no histological findings are pathognomonic for PSC . Frequent findings include :
- periductal fibrosis (onion skin lesions)
- periportal eosinophilic infiltrate
- paucity of ducts
Associations
- ulcerative colitis
- 70-80% of patients with PSC develop inflammatory bowel disease
- 87% of these develop ulcerative colitis
- 70-80% of patients with PSC develop inflammatory bowel disease
- autoimmune hepatitis (AIH-PSC overlap)
- Sjogren syndrome
- retroperitoneal fibrosis
- mediastinal fibrosis
- Riedel thyroiditis
- orbital pseudotumor
Complications
Markers
Unlike primary biliary cholangitis, antibody titers are usually absent or low . Liver function tests will usually have a cholestatic pattern with elevated alkaline phosphatase (ALP) and bilirubin .
Radiographic features
The entire biliary tree (both intra and extrahepatic) may be involved, with multiple strictures scattered along its length. In ~20% only the intrahepatic and proximal extrahepatic bile ducts are involved.
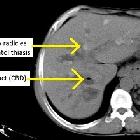
The end result of PSC is cirrhosis which is usually characterized by a markedly distorted biliary tract and atrophy of the entire liver with the exception of the caudate lobe which is hypertrophied in almost all cases (68-98%) . Atrophy involving the left lobe is a feature which somewhat distinguishes it from cirrhosis from other causes, in which the left lobe is usually hypertrophied .
Ultrasound
Ultrasound is able to demonstrate both the changes of cirrhosis and irregularity of bile duct caliber. Additionally, brightly echogenic portal triads may be visible.
PSC is a risk factor for developing gallbladder cancer, so gallbladder polyps should be considered malignancy until proven otherwise.
CT
- contour abnormalities and atrophy (see above)
- marked caudate lobe hypertrophy
- the atrophied liver is of lower density than the hypertrophied caudate lobe
- multiple linear discontinuous low-density regions representing dilated intrahepatic bile duct segments
MRCP & ERCP
ERCP has traditionally been the gold standard for the depiction of the biliary tree, and also offers the ability to perform cholangioplasty, if necessary. In practice, however, MRCP is used before ERCP since it is noninvasive, can visualize the liver, and it avoids the 10% risk of hospitalization from ERCP in PSC patients .
The characteristic findings on direct imaging of the biliary tree are :
- multiple segmental strictures
- typically short segment
- intervening segments are of normal caliber or slightly dilated (beading)
- biliary dilatation: may be present in ~85% of cases
- general: ~35%
- segmental: ~50%
- biliary diverticula
- mural irregularities
- distortion of the biliary tree due to associated cirrhosis
Treatment and prognosis
The only cure available at present is orthotopic liver transplantation (OLT) with 5-year survival rates approaching 80% . However, there is evidence that PSC may recur in 5-20% of patients post-transplantation .
No medical therapy has stood the test of time, with ursodeoxycholic acid, immunosuppression, chelation and antifibrolytic therapy unable to demonstrate consistent benefits over placebo .
Percutaneous cholangioplasty of dominant strictures is usually performed in a retrograde fashion via ERCP or via a transhepatic approach .
Complications
- cholangiocarcinoma develops in ~15% patients
- colorectal cancer
- 4x greater risk compared to IBD patients without PSC
- 10x greater risk compared to general population
- hepatocellular carcinoma: appears to be not increased beyond other causes of cirrhosis
Differential diagnosis
General imaging differential considerations include:
- cirrhosis from other causes
- caudate lobe not as frequently or as markedly enlarged
- left lobe usually also hypertrophied
- IgG4-related sclerosing cholangitis
- these patients tend to be older and more symptomatic with involvement of other systems besides the bile ducts
- IgG4 levels 4x normal; ratio of IgG4 to immunoglobulin 1 of >0.24
- responds to steroid therapy
- secondary sclerosing cholangitis
- AIDS-associated cholangitis
- biliary strictures from other causes, e.g. surgery, ischemia
- cholangiocarcinoma (can also occur as a later complication)
- primary biliary cirrhosis
- especially difficult to distinguish when PSC is limited to the intrahepatic biliary tree
- young women more frequently affected
- high antibody titers
- Alagille syndrome (arteriohepatic dysplasia)
- hepatic sarcoidosis: see abdominal manifestations of sarcoidosis
Siehe auch:
- Leberzirrhose
- cholangiozelluläres Karzinom
- abdominelle Manifestationen der Sarkoidose
- Alagille-Syndrom
- Hepatolithiasis
- Gallengangsstrikturen
- primär biliäre Cholangitis
- PSC und Morbus Crohn
- Primär sklerosierende Cholangitis und Colitis ulcerosa
- IgG4-assoziierte Cholangitis
- AIDS associated cholangitis
und weiter:


 Assoziationen und Differentialdiagnosen zu Primär sklerosierende Cholangitis:
Assoziationen und Differentialdiagnosen zu Primär sklerosierende Cholangitis:





