Tumoren der Wirbelsäule

Bone up on
spinal osseous lesions: a case review series. Summary of the lesions discussed in this article with their characteristic imaging and clinical findings
Bone up on
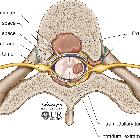
spinal osseous lesions: a case review series. Classification of spinal tumors by location. Spinal neoplasms can be classified according to their anatomic locations, specifically extradural, extramedullary-intradural, and intramedullary tumors

Bone up on
spinal osseous lesions: a case review series. Spinal metastases. Sagittal MR images demonstrate numerous ill-defined lesions throughout the lumbar spine (arrows). These lesions demonstrate low signal on the T1-weighted sequence (a), intermediate to high signal on the T2 -weighted sequence (b), and heterogenous contrast enhancement on the post-contrast T1 fat-saturated sequence (c)

Pitfalls in
the diagnosis of common benign bone tumours in children. Aneurysmal bone cyst of the second cervical vertebra (C2): a Lateral X-ray of the cervical spine: large expansile lytic lesion of the posterior arch C2 (between arrowheads). b CT, axial slice, bone windowing: confirmation of the lesion, with extreme thinning and focal interruption of the bone cortex. c CT, axial slice, soft-tissue windowing: fluid-fluid levels (arrows) are identified inside the cyst

Bone up on
spinal osseous lesions: a case review series. Angiosarcoma. Axial CT image in the bone window (a) demonstrates a large lytic lesion replacing the majority of the sacrum (orange arrow), with multiple areas of cortical erosion and destruction (white arrows). In the contrast-enhanced soft tissue window (b), enhancing areas are present within the mass, representing serpiginous vessels (black arrows). T2 weighted MR image (c) of the lumbosacral spine demonstrates a heterogeneous, destructive mass within the sacrum (orange arrows), with extension into the paraspinal soft tissues. The mass is low to intermediate signal on pre-contrast T1-weighted imaging (d). Post-contrast T1-weighted fat-suppressed image (e) demonstrates heterogeneous enhancement

Bone up on
spinal osseous lesions: a case review series. Ewing’s sarcoma. Axial CT image in the bone window (a) demonstrates an ill-defined lesion with destructive changes of the right vertebral body. The bone cortex has a “smudged” appearance (black arrow) due to perforation of tumor through the cortex. Sagittal proton-density image (b) demonstrates the ill-defined tumor as abnormal marrow signal with epidural extension (orange arrows). Sagittal T2-weighted (c) and T2 fat-saturated (d) images demonstrate variable signal within the lesion (orange arrows). This lesion demonstrates low to intermiediate T1 signal (e, orange arrows). On T1-weighted post-contrast imaging (f), there is heterogenous enhancement of the tumor (orange arrows), which is difficult to distinguish from the enhancing peritumoral edema (white arrow)

Bone up on
spinal osseous lesions: a case review series. Osteosarcoma. Axial bone window CT image (a) demonstrates moth-eaten destruction of the right lateral mass of C1 (arrow), with a wide zone of transition along the posteromedial margin. Sagittal (b) and axial (c) T2-weighted images demonstrate the lesion to be low to intermediate in signal (arrow). The lesion is also low signal on T1-weighted images (d, e), and demonstrates avid enhancement (arrows) on post-contrast T1 sequences (f, g)

Bone up on
spinal osseous lesions: a case review series. Chondrosarcoma. Axial CT image in the soft tissue window (a) demonstrates a mass centered at the left paravertebral region with expansile ring and arc calcifications (arrows), typical of a chondroid tumor matrix. On sagittal off-midline CT image (b), the tumor is seen extending over multiple vertebral levels. Sagittal GRE image (c) demonstrates areas of low signal within the tumor, due to its calcific components. Sagittal T1-weighted image (d) demonstrates variable signal intensity of the tumor. Axial T2-weighted image (e) demonstrates lobular, predominantly high signal intensity of the tumor due to the high-water content of hyaline cartilage. Additionally, there is epidural extension of the tumor (black arrow), displacing the spinal cord. Peripheral areas of low signal intensity are due to calcifications. The T1 fat-suppressed post-contrast image (f) demonstrates enhancement along the periphery and internal septa (white arrows). The non-enhancing areas represent hyaline cartilage, cystic mucoid tissue and necrosis

Bone up on
spinal osseous lesions: a case review series. Chordoma. Sagittal T2-weighted (a), axial T2-weighted fat-saturated (b), and coronal T2-weighted (c) images demonstrate a heterogeneously hyperintense, expansile and destructive lesion (orange arrows) involving the L3 vertebral body. Numerous internal septa (white arrows) are seen within the lesion, creating a “honeycomb” configuration. The lesion extrudes out and over the left aspect of the veretebral body (creating a "mushroom" appearance), and displaces the adjacent paraspinal musculature

Bone up on
spinal osseous lesions: a case review series. Lymphoma. Axial CT images through the lumbar spine (a) and sacrum (b) demonstrate abnormal soft tissue within the spinal canal (black arrows). Additionally, there is soft tissue replacement of the normal fat in the right sacral foramen (orange arrow). T2-weighted MR image (c) of the lumbosacral spine demonstrates an intermediate to low signal lesion involving the posterior aspect of L5, and another component at S1-S2 (orange arrows). There is no involvement of the intervertebral discs. Post-contrast T1-weighted fat-suppressed image (d) demonstrates relatively homogeneous enhancement

Bone up on
spinal osseous lesions: a case review series. Plasmacytoma. Sagittal and axial MR images demonstrate an expansile mass (orange arrows) arising from the posterior elements of C2 and C3. The mass demonstrates hypointense signal to normal marrow on T1 (a), and isointense to hyperintense signal on T2 (b). Post-contrast sagittal T1 (c) and axial T1 fat-suppressed (d) sequences demonstrate enhancement. A few areas of curvilinear low-signal intensity are seen at the remaining thickened bony cortex (white arrows), projecting into the lesion, resulting in a “mini-brain” appearance resembling cortical sulci

Bone up on
spinal osseous lesions: a case review series. Pyogenic spondylodiskitis. Sagittal STIR image (a) demonstrates abnormal marrow signal of C2, C3, C5, C6, and C7 (asterisks) with diffuse paravertebral soft tissue edema. Post-contrast T1-weighted image (b) demonstrates corresponding marrow enhancement, disc enhancement, and endplate erosion (orange arrows). Phlegmon or abscesses are seen at the level of C2-C3, C5-C6, and C6-C7 (white arrows), as well as epidural phlegmon extending along the dorsal aspects of C2 to C7. Sagittal T2 image (c) demonstrates fluid signal within the disc at C2-C3 and C5-C6 (black arrows), characteristic of pyogenic spondylodiskitis

Bone up on
spinal osseous lesions: a case review series. Compressive vertebral venous vascular malformation. Sagittal (a) and axial (b) CT images in the bone window of the thoracic spine demonstrate decreased attenuation of the T4 vertebral body, as well as the left pedicle and transverse process. A characteristic “polka-dot” sign is seen in the vertebral body on the axial image, with high attenuation dots representing replacement of normal cancellous bone by thick, vertical trabeculae (orange arrows) surrounded by vascular lacunes and fatty marrow. Sagittal MR images demonstrate a heterogenous, predominantly high signal lesion on both T1 (c) and T2 (d) weighted sequences involving the T4 vertebral body (orange arrows), with lobular extension into the spinal canal (white arrows). Axial T1 pre- (e) and post-contrast (f) images demonstrate avid enhancement of the lesion. Again, there is extension of the lesion from the vertebral body into the spinal canal, with resulting compression of the spinal cord

Bone up on
spinal osseous lesions: a case review series. Eosinophilic granuloma. Sagittal T1 image (a) demonstrates suggestion of vertebral plana (orange arrow), however difficult to detect due to the lesion appearing isointense to pediatric marrow on T1. Sagittal T1 post-contrast MR image (b) shows an enhancing mass (orange arrows) with diffuse marrow infiltration of C5 and C7 (white arrows), and C6 pathologic vertebral collapse, sparing the adjacent vertebral endplates and discs. Sagittal T2 (c) and T2 fat -saturated (d) images demonstrate the lesion as a heterogeneously hyperintense soft tissue mass. There is edema of the posterior interspinous soft tissue, more evident on fat suppressed image (blue arrows). Axial T1 post contrast image (e) demonstrates asymmetric enhancement surrounding the right facets (orange arrow)

Bone up on
spinal osseous lesions: a case review series. Giant cell tumor. Sagittal (a) and axial (b) CT images demonstrate a well-defined, expansile lytic lesion involving the right posterolateral aspect of the T10 vertebral body and right pedicle. No discrete sclerotic rim is seen around the lesion margins. Sagittal and axial MR images demonstrate a homogenous, well defined mass (orange arrows) in the posterior aspect of T10, with low signal on T1- (c, d) and low to intermediate signal characteristics on T2- (e) weighted sequences. A trace amount of increased signal is seen in the adjacent marrow, consistent with mild marrow edema (white arrows)

Bone up on
spinal osseous lesions: a case review series. Aneurysmal bone cyst. MRI imaging in the same patient as Fig 9. Pre-contrast axial T1-weighted image (a) confirms fluid-fluid levels within the lesion (orange arrows), indicating hemorrhage with sedimentation of varying stages of blood products. Post-contrast axial T1-weighted image (b) demonstrates enhancement of the septa within the lesion (orange arrows). Note a partially hypointense rim, representing cortex (white arrow). Axial T2-weighted image (c) re-demonstrates a destructive lesion with fluid-fluid levels (orange arrows); varying signal intensity corresponds to differing stages of blood product degradation

Bone up on
spinal osseous lesions: a case review series. Aneurysmal bone cyst. Lateral radiograph (a) of the cervical spine demonstrates a large, osteolytic, expansile mass arising from the C2 vertebral body, resulting in significant bony remodeling. The mass is sharply defined and demonstrates thin sclerotic margins, also known as an “eggshell cortex” (orange arrows). Sagittal CT image of the cervical spine (b) confirms the lesion within the C2 vertebral body. Axial CT image in the soft tissue window (c) shows fluid-fluid levels (orange arrows), compatible with hemorrhage. Axial CT image in the bone window (d) shows near complete obliteration of the posterior arch with some areas of remnant thin sclerotic rim, "eggshell cortex" (white arrow)

Bone up on
spinal osseous lesions: a case review series. Osteoblastoma. Sagittal T1 weighted MR image (a) demonstrates a low signal lytic lesion involving the T10 vertebral body and posterior elements (orange arrows). The lesion is intermediate to high signal on T2 weighted images (b, c). There is an associated T2 hyperintense component, consistent with an aneurysmal bone cyst (white arrow), which can be seen in 10-20% cases of osteoblastomas

Bone up on
spinal osseous lesions: a case review series. Osteoblastoma. Axial (a) CT image of the thoracic spine demonstrates a lytic lesion involving the T7 vertebral body (orange arrow) and posterior elements, with an expansile soft tissue component. A thin sclerotic rim can be seen along the border of the intervertebral portion of the lesion (white and black arrows). Sagittal T2 (b), T1 pre-contrast (c), and T1 post-contrast (d) MR images again demonstrate a lesion involving the T7 vertebral body and posterior elements (orange arrows), as well as invasion of the adjacent paraspinal soft tissues. The lesion is predominantly low to intermediate signal compared to normal marrow, and demonstrates avid enhancement on post-contrast images

Bone up on
spinal osseous lesions: a case review series. Osteoid osteoma. Axial CT image (a) demonstrates a 1.2-cm sclerotic nidus (asterisk) at T10. The lesion is sharply demarcated with surrounding reactive sclerosis (arrow). Nuclear medicine bone scan (b) demonstrates focal intense uptake at T10 corresponding within the lesion (arrow)

Bone up on
spinal osseous lesions: a case review series. Enostosis with adjacent vertebral vascular malformation. Axial CT image of the spine (a) demonstrates the enostosis as a sclerotic bone lesion (white arrow). MRI shows low signal intensity like cortical bone; hypointensity on T1- (d, white arrow) and T2- (b, white arrow) weighted images, without enhancement post contrast (c, e). There is an adjacent ill-defined lesion with lucencies and intervening thickened trabeculae (a, orange arrows). This lesion demonstrates T1/T2 hyperintense signal (b, d, orange arrows), fat suppression (c, e, orange arrows) and no enhancement post contrast (c, e, orange arrow). This lesion is consistent with a vertebral venous vascular malformation (formerly known as a hemangioma)

Bone up on
spinal osseous lesions: a case review series. Enostosis. Axial CT image (a) of the thoracic spine demonstrates a focal sclerotic bone lesion with characteristic dense sclerosis and irregular and brush-like margins (arrow). No associated soft tissue component. Axial fused PET/CT image (b) demonstrates lack of metabolic activity of the bone lesion (arrow), confirming the diagnosis

Bone up on
spinal osseous lesions: a case review series. Vertebral venous vascular malformation. Sagittal (a) and axial (b) T2-weighted MR images demonstrate a well-defined lesion in the right posterolateral aspect of T12 (arrows). The lesion is hyperintense relative to the surrounding normal marrow, and demonstrates suppression (arrow) on the T2 fat-suppressed sequence (c). This was an incidental finding and diagnosed radiographically as a vascular malformation. Given the lack of expansion into the spinal canal or compression of the cord, unlike the prior case, this is considered a “do not touch” lesion

Ewing sarcoma
• Ewing sarcoma - C1 - Ganzer Fall bei Radiopaedia
The differential diagnosis for a vertebral body mass is broad and may range from a completely benign, sclerotic enostosis (bone island) to a malignant primary bone tumor.
Classification
Broadly, these lesions can be separated into:
- non-neoplastic lesions
- primary bone tumors
- secondary metastatic disease
Non-neoplastic lesions
- aneurysmal bone cyst (<2%)
- neural arch (60%); vertebral body (40%)
- Brown tumor (an osteoclast reaction in hyperparathyroidism)
- enostosis
- vertebral hemangioma
Primary bone tumors
Primary bone tumors of the spine are much less common than secondary metastatic disease:
- plasmacytoma/multiple myeloma
- most common primary bone cancer
- chordoma
- chondrosarcoma
- Ewing sarcoma
- lymphoma
- osteosarcoma
- giant cell tumor
- osteoblastoma
- osteochondroma
- Langerhans cell histiocytosis (eosinophilic granuloma)
- vertebral body; can cause vertebra plana
- osteoid osteoma
- neural arch predominance
Secondary metastatic disease
Vertebral metastases are significantly more common than primary bone tumors, especially in an older patient or one with known primary disease elsewhere.
Assessment of whether the bone lesions are sclerotic or lytic may help to narrow the differential diagnosis of primary disease if it is unknown.
Siehe auch:
- Hämangiom der Wirbelsäule
- kartilaginäre Exostose
- Multiples Myelom
- Pleomorphes Undifferenziertes Sarkom
- skeletale Manifestationen der Langerhanszell-Histiozytose
- Ostitis fibrosa cystica
- sacrococcygeales Chordom
- Riesenzelltumor der Wirbelsäule
- Osteoblastom der Wirbelsäule
- Osteoidosteom der Wirbelsäule
- Aneurysmatische Knochenzyste der Wirbelsäule
- Tumoren der Halswirbelsäule
- Osteosarkom Wirbelsäule
- Angiosarkom der Wirbelsäule
- Ewingsarkom der Wirbelsäule


 Assoziationen und Differentialdiagnosen zu Tumoren der Wirbelsäule:
Assoziationen und Differentialdiagnosen zu Tumoren der Wirbelsäule:







skeletale
Manifestationen der Langerhanszell-Histiozytose

