pulmonary and mediastinal manifestations sarcoidosis


























































Pulmonary and mediastinal involvement of sarcoidosis is extremely common, seen in over 90% of patients with sarcoidosis. Radiographic features are variable depending on the stage of the disease.
For a general discussion, please refer to the parent article: sarcoidosis.
Epidemiology
Pulmonary manifestations are present in ~ 90% of patients. Patients between 20 and 40 years of age are most commonly affected, although lung involvement can be seen at any age . There is a slight female predominance, particularly among African-Americans. It is rare in Asians.
Clinical presentation
Clinical presentation is variable. Approximately 50% of patients are asymptomatic. The remainder present with either respiratory symptoms (e.g. cough and dyspnea) or skin changes (e.g. erythema nodosum, lupus pernio, scars, plaques) .
Löfgren syndrome is an uncommon but specific acute presentation with a better prognosis.
Respiratory function tests tend to demonstrate a restrictive pattern with reduced lung volumes and reduced diffusion capacity. Obstructive components are usually seen in patients who also smoke, and are primarily attributable to the later .
Pathology
Sarcoid granulomata mainly occur in a distribution along the lymphatics in the bronchovascular sheath and, to a lesser extent, in the interlobular septa and subpleural lung regions. This distribution is one of the most helpful features in recognizing sarcoidosis pathologically and is responsible for the high rate of success in diagnosis by bronchial and transbronchial biopsies .
Thus, on gross examination, multiple pulmonary granulomas occur in a characteristic lymphatic and perilymphatic distribution. Microscopically, the granulomas are typically non-caseating and coalescent.
The granulomas may resolve spontaneously or progress to fibrosis.
Radiographic features
Both chest radiograph and CT are commonly used to evaluate for thoracic sarcoidosis. Imaging evaluation can be tricky, as the manifestations are variable and depend on the stage of disease on both x-ray and CT . In addition, it is essential to understand that imaging findings are non-specific or atypical in 25-30% - sarcoidosis is often termed the "great mimicker" .
Although there is a large spectrum of thoracic imaging findings, the most typical manifestations include:
- symmetric hilar and mediastinal lymphadenopathy (>75%)
- distribution
- hilar nodes almost always involved (isolated middle mediastinal adenopathy rare)
- unilateral hilar enlargement without mediastinal involvement rare (1-3%)
- isolated anterior/posterior nodal enlargement uncommon - almost always occurs in combination with middle mediastinal and hilar involvement
- atypical patterns more common in patients presenting ≥50 years of age
- usually without mass effect on adjacent structures (e.g. vessels)
- +/- nodal calcification
- cluster of black pearls sign
- distribution
- wide spectrum of pulmonary parenchymal changes:
- perilymphatic micronodules
- airspace opacities/consolidation (e.g. alveolar sarcoidosis) - less common
- lung masses - less common
- pulmonary fibrosis
- pleural effusion(s)
- usually small or moderate in size
- usually, resolve within 2-3 months
Plain radiograph
Chest x-ray is less sensitive than CT for thoracic manifestations of sarcoidosis. The radiograph may appear normal despite the presence of pulmonary granulomas histologically (5-10% of cases). The Scadding criteria have been used, despite limitations, to stage sarcoidosis for decades.
Patterns of lymphadenopathy include:
- 1-2-3 sign or Garland triad
- classic nodal constellation reflects relatively high sensitivity of chest x-ray for adenopathy in these nodal stations. Left paratracheal and aortopulmonary nodes also frequently enlarged, but harder to identify
- nodes can be very large, but tend not to abut the cardiac silhouette
- as opposed to lymphoma, in which nodes may be continuous with the pericardial outline
- calcification
- up to 20% of intrathoracic nodes calcify after ten years
- pattern is variable: punctate, amorphous or eggshell (5%)
Patterns of pulmonary disease on plain radiograph include:
- reticulonodular opacities
- most common: 75-90% of stage II and III cases
- middle and upper zone distribution
- bilateral and symmetric
- nodularity may be prominent, resembling miliary opacities (miliary sarcoidosis)
- airspace opacities: alveolar sarcoidosis (atypical)
- may present with ill-defined and peripheral, and represents interstitial rather than an intra-alveolar process
- nodules: nodular pulmonary sarcoidosis (rare)
- masses (sarcoid galaxy sign)
- more frequent in patients older than 50 years of age at presentation
- rarely solitary
- coalescence of multiple ill-defined nodules
- peripheral cavitation: cavitatory pulmonary sarcoidosis (rare)
- more common in necrotizing sarcoid granulomatosis
- must rule out superinfection with tuberculosis
- pulmonary fibrosis (end stage disease, 20-25%)
- most commonly at upper and middle lung zones
- permanent coarse linear opacities, often radiating laterally from the hilum upward and outward elevation of hila
- traction bronchiectasis
CT
Although chest x-ray may be sufficient for the diagnosis, CT or high-resolution CT provides better evaluation of lung changes and lymphadenopathy, as well as corollary findings such as pulmonary artery enlargement or sequela of cystic disease (e.g. mycetoma formation). Consequently, CT allows a more accurate correlation to disease stage and pulmonary function tests. It may be especially useful in patients with normal (stage 0) or isolated nodal involvement (stage I) by chest x-ray .
CT is more sensitive for characteristic hilar/mediastinal lymphadenopathy of sarcoidosis (80-90%).
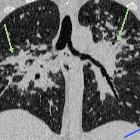
Parenchymal findings on CT include :
- perilymphatic irregular nodular thickening in an upper/mid lung distribution
- central interstitium: bronchovascular bundles including centrilobular nodules
- peripheral interstitium: interlobular septa, subpleural lung and interlobar fissures
- small nodules may dominate and appear similar to miliary opacities
- nodules or large opacities measuring 1 to 4 cm
- confluence of many smaller nodules, thus irregular margins
- seen in 15 to 25% of patients
- may mimic consolidation
- frequently contain air bronchograms
- ground-glass opacities
- represent extensive interstitial sarcoid granulomas below the resolution of HRCT rather than alveolitis
- features of small airways disease
- due to a granulomatous bronchiolitis
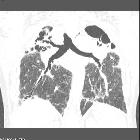
- pulmonary fibrosis
- represents stage IV disease
- three main patterns described corresponding to pulmonary function testing results :
- central bronchial distortion or bronchiectasis featuring air trapping, with predominantly obstructive physiology
- peripheral honeycombing, with predominantly restrictive physiology and low DLCO:
- usually a minor feature and present only in severe fibrosis
- subpleural
- mainly the middle and upper lung zones
- lower lobes predominance resembling UIP is rare
- diffuse linear fibrotic pattern, with more mild effect on respiratory function
- typically radiate away from hila in all directions
- the pattern of distortion of lung architecture may be mixed:
- traction bronchiectasis
- compensatory hyperinflation of the lower lobes
- upward and outward retraction of hila
- posterior displacement of the upper lobe bronchi, indicating loss of volume in the posterior segments of the upper lobes
- adjacent to areas of dense fibrosis, likely to represent paracicatricial emphysema
- patchy air trapping at the level of the secondary lobules
- air trapping is presumably secondary to bronchiolar obstruction by submucosal granulomas
- much more pronounced in patients who are also smokers
Pleural involvement is infrequent :
- pleural effusion (bland, chylous, hemorrhagic)
- pleural thickening/plaques
Tracheal or bronchial involvement is only rarely seen but may result in stenosis .
Nuclear medicine
PET-CT
Sarcoidosis is characteristically FDG-avid, and PET-CT has been shown to have high sensitivity (94-100%) for thoracic disease . Thus, FDG-PET-CT may be useful for :
- identification of occult sites of disease
- identifying a suitable target for diagnostic biopsy
- gauging active inflammatory disease in patients with prolonged symptoms
- assessing response to treatment
Scintigraphy
Gallium-67 scintigraphy usually shows high uptake in active sarcoidosis and is useful for assessing disease activity and response to treatment, although as it is a non-specific marker of inflammation, it is non-specific. It has a role also in detecting extrathoracic involvement (see sarcoidosis) .
The gallium equivalent of 1-2-3 sign or Garland triad is known as the lambda sign.
Treatment and prognosis
Treatment is predominantly with corticosteroids, which are usually administered only to patients with active disease. Unfortunately distinguishing active disease superimposed on chronic fibrotic changes is difficult and criteria are controversial .
Pulmonary involvement is responsible for the majority of morbidity and mortality in patients with sarcoidosis. The overall mortality rate is approximately 5%, with patients who present insidiously faring worse than those who present with an acute onset . Likelihood of resolution depends on the stage of disease at presentation :
- stage I: 60% resolution within 1-2 years
- stage II: 46%
- stage III: 12%
Complications
Recognized complications include :
- pulmonary fibrosis (stage IV)
- vascular compression
- pulmonary arterial hypertension and cor pulmonale
- pulmonary venous / venoatrial compression
- aspergillomas complicated by hemoptysis
Differential diagnosis
The differential often depends on the stage of disease and particular appearances:
- stage I: differential of intrathoracic nodal enlargement
- stage III:
- stage IV:
- differential of pulmonary fibrosis
- differential of egg-shell calcification


 Assoziationen und Differentialdiagnosen zu thorakale Sarkoidose:
Assoziationen und Differentialdiagnosen zu thorakale Sarkoidose:













