akute Pyelonephritis



















Acute pyelonephritis (plural: acute pyelonephritides) is a bacterial infection of the renal pelvis and parenchyma most commonly seen in young women. It remains common and continues to have significant morbidity in certain groups of patients.
Epidemiology
The incidence of acute pyelonephritis parallels that of lower urinary tract infections: approximately five times more common in females with a sharp increase following puberty .
Clinical presentation
Clinical presentation is fairly specific and classical in most cases, consisting of a rapid onset of high fever, flank pain and costovertebral angle tenderness (i.e. positive Murphy kidney punch). In many instances, less specific or non-urinary symptoms and signs may also be present, which may lead to clinical confusion .
White cells and bacteria are usually present in the urine, and blood tests reveal the expected changes: leucocytosis and increased C-reactive protein (CRP) and/or erythrocyte sedimentation rate (ESR). In severe cases, sepsis may be present.
Pathology
The most commonly implicated organisms are from the gastrointestinal tract :
- Escherichia coli (most common)
- Klebsiella spp.
- Proteus spp.
- Enterobacter spp.
- Pseudomonas spp.
- Haemophilus influenzae
Infection gains access to the upper urinary tract by passing retrograde up the ureter from the bladder, facilitated by virulence factors which allow bacteria to adhere to the urothelium (e.g. adhesin P) and inhibit ureteric peristalsis (endotoxins) . The infection then passes into the collecting tubules and results in an interstitial nephritis, with resulting alterations in renal filtration and blood flow in the affected region. Localised ischaemia secondary to inflammatory changes results in altered imaging and may eventually lead to necrosis and scar .
Rarely, the kidney may be seeded haematogenously, in which case renal abscesses develop rather than pyelonephritis. These abscesses usually develop peripherally.
Radiographic features
In many instances, the clinical presentation suffices for making the diagnosis. Situations in which imaging is indicated include:
- exclude obstructed kidney
- high-risk patients: diabetics, elderly, immunocompromised
- those with a mixed clinical picture
- previous renal pathology
Plain radiograph
Radiography has a limited role, especially if patients are likely to go on to CT. Abdominal radiographs may demonstrate obstructing urinary tract calculi and occasionally may demonstrate gas within the collecting system (emphysematous pyelonephritis).
Ultrasound
Ultrasound is insensitive to the changes of acute pyelonephritis, with most patients having 'normal' scans. Abnormalities are identified in only ~25% of cases . Possible features include:
- particulate matter/debris in the collecting system
- reduced areas of cortical vascularity by using power Doppler
- gas bubbles (emphysematous pyelonephritis)
- abnormal echogenicity of the renal parenchyma
- focal/segmental hypoechoic regions (in oedema) or hyperechoic regions (in haemorrhage)
- mass-like change
Ultrasound is, however, useful in assessing for local complications such as hydronephrosis, renal abscess formation, renal infarction, perinephric collections, and thus may guide management.
CT
CT is a sensitive modality for evaluation of the renal tract, able to assess for renal calculi, gas, perfusion defects, collections and obstruction. Unfortunately, it does have a significant radiation burden and should be used sparingly, especially in young patients.
There is usually no need for a three or four phase CT IVP (CT urography). A single 45-90 second post-contrast scan usually suffices, although clinical acumen may be necessary to choose the best contrast phase . For example, if renal colic is suspected then a non-contrast scan is often required to assess for renal calculi. If renal ischaemia is suspected then an arterial scan (15-25 seconds) is ideal to assess perfusion .
Non-contrast CT
- often the kidneys appear normal
- affected parts of the kidney may appear oedematous, i.e. swollen and of lower attenuation
- renal calculi or gas within the collecting system may be evident
- perinephric stranding: although not considered a useful sign
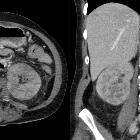
Post-contrast CT
- one or more focal wedge-like regions will appear swollen and demonstrate reduced enhancement compared with the normal portions of the kidney
- the periphery of the cortex is also affected, helpful in distinguishing acute pyelonephritis from a renal infarct (which tends to spare the periphery; the so-called 'rim sign')
- if imaged during the excretory phase, a striated nephrogram may also be visible
If for some reason the kidney is imaged again within 3-6 hours, persistent enhancement of the affected regions may be evident due to slow flow of contrast through the involved tubules .
MRI
MRI is usually reserved for patients who are pregnant, and findings mirror those seen on CT. The kidney demonstrates wedge-shaped regions of altered signal:
- T1: affected region(s) appear hypointense compared with the normal kidney parenchyma
- T2: hyperintense compared to normal kidney parenchyma
- T1 C+: reduced enhancement
A fast inversion recovery sequence obtained after contrast administration has been shown to be particularly effective in outlining affected regions which appear hyperintense compared to the low signal parenchyma. The contrast is thought to represent a combination of local oedema and decreased T2 signal due to gadolinium in the perfused 'normal' portions .
Nuclear medicine
Technetium-99m dimercaptosuccinic acid (DMSA) demonstrates a similar reduction in renal perfusion and function, which appears as one or more patchy scintigraphy defects in the outline of the kidneys .
Treatment and prognosis
Most patients respond rapidly to appropriate antibiotic therapy, and often no imaging whatsoever is required.
Even when imaging has been performed, no follow-up imaging is usually required, unless patients do not respond clinically, and it should be stressed that imaging changes can take up to five months to resolve .
The presence of an upper urinary tract infection in the presence of obstruction can threaten the viability of the kidney and a percutaneous nephrostomy is usually required on an emergency basis.
Complications
Complications include :
- lobar nephronia
- renal abscess
- renal infarction, necrosis and scarring
- chronic renal impairment
- hypertension
- renal vein thrombosis
- in pregnancy: septic shock and premature labour
Differential diagnosis
General imaging differential considerations include:
- renal infarction
- typically spares the peripheral aspect of the cortex, giving the cortical rim sign
- other causes of interstitial nephritis
- sarcoidosis
- drug-induced
- renal lymphoma: has multiple presentations and can mimic pyelonephritis
Practical points
- CT is the most sensitive modality for diagnosis and assessment of complications
- CT portal venous phase demonstrating areas of reduced enhancement compared with the normal portions of the kidney is the key for diagnosis
- striated nephrogram on CT excretory phase
- evidence of obstruction in the setting of pyelonephritis/sepsis is a medical urgency requiring percutaneous nephrostomy
Siehe auch:
- Sarkoidose
- Niereninfarkt
- Pyelonephritis
- akute bakterielle Nephritis
- cortical rim sign
- Pseudotumor der Niere
- Nephritis
- fleckige Nierenkontrastierung
- Urosepsis
- akutes Nierenversagen mit Lendenschmerz und fleckiger Vasokonstriktion der Nieren
- chronische Pyelonephritis
und weiter:


 Assoziationen und Differentialdiagnosen zu akute Pyelonephritis:
Assoziationen und Differentialdiagnosen zu akute Pyelonephritis:



