atrial septal defect (ASD)






























Atrial septal defect (ASD) is the second most common congenital heart defect after ventricular septal defects and the most common to become symptomatic in adulthood.
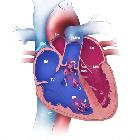
They are characterized by an abnormal opening in the atrial septum allowing communication between the right and left atria. Due to the low pressures of the atria, the lesion is typically asymptomatic until adulthood despite 2-4 times the normal pulmonary blood flow. Gradual (high output) congestive cardiac failure eventually develops, usually becoming symptomatic by the age of 30.
Epidemiology
Atrial septal defects account for ~10% of congenital heart disease . There may be greater female predilection.
Associations
Atrial septal defects are seen in association with the following:
- Down syndrome (ostium primum defect)
- Holt-Oram syndrome
- Ellis-van Creveld syndrome
- mitral valve prolapse
- Lutembacher syndrome
- anomalous pulmonary venous return (especially with sinus venosus defects)
Clinical presentation
Most patients are asymptomatic but as cardiac failure develops they may present with shortness of breath, palpitations, and weakness . Chest auscultation classically reveals an ejection systolic murmur heard at the left upper sternal border, attributed to increased flow across the pulmonary valve rather than blood shunting across the defect itself .
ECG
- incomplete right bundle branch block (RBBB morphology with QRS duration between 110-120 ms)
- increased specificity with crochetage sign in the inferior (II, III, aVF) leads
- right precordial (V1-3) "defective T waves"
- describes biphasic morphology, initial T wave flattening or inversion and sharp, positive upstroke to terminal positive deflection
- peak of the T wave delayed when compared to lateral precordial leads
- notching of the terminal upstroke of the R wave (crochetage sign) correlates with the size of ASD and implies a greater degree of shunting
- left axis deviation
- characteristic of ostium primum defects and anatomical distortion of the left bundle branch fascicles
- associated first degree AV block
- right axis deviation
- suggests ostium secundum defect
- low atrial ectopic rhythms
- negative P wave polarity in lead II
- found in sinus venosus ASDs
Pathology
Classification
There are four major types of atrial septal defect (ASD) , distinguished according to their location within the septum:
- secundum ASD
- 60-90% of all ASDs
- usually an isolated abnormality
- primum ASD
- 5-20%
- associated with cleft anterior mitral valve leaflet (partial atrioventricular septal defect)
- sinus venosus
- 5%
- associated with anomalous right pulmonary venous return to the superior vena cava or right atrium
- coronary sinus type ASD ("unroofed coronary sinus")
- <1%
- see: unroofed coronary sinus
A patent foramen ovale (PFO) is a form of atrial septal defect.
Radiographic features
Plain radiograph
- can be normal in early stages when the atrial septal defect is small
- signs of increased pulmonary flow (pulmonary plethora or shunt vascularity)
- enlarged pulmonary vessels
- upper zone vascular prominence
- vessels visible to the periphery of the film
- eventual signs of pulmonary arterial hypertension
- chamber enlargement
- right atrium
- right ventricle
- note: left atrium is normal in size unlike VSD or PDA
- note: aortic arch is small to normal
Treatment and prognosis
Atrial septal defects do not cause any impairment in cardiac function in utero and even most neonates are asymptomatic. The defect can be closed surgically or percutaneously (e.g. atrial septal occlusion device). However, careful evaluation has to be made to ensure lack of development of elevated right heart pressures or a right to left shunt before any intervention.
Complications
In approximately 10% of untreated patients, pulmonary hypertension develops. In this situation, flow through the shunt eventually reverses and becomes right to left. The patient then becomes cyanotic. This is known as Eisenmenger syndrome.
Other complications include:
- paradoxical emboli
- cardiac conduction defects, e.g. atrial fibrillation, flutter
Siehe auch:
- Herzfehler
- Kardiomegalie
- pulmonale Hypertonie
- Aortenbogen
- persistierendes Foramen ovale
- Vena cava superior
- Ellis-van-Creveld-Syndrom
- totale Lungenvenenfehlmündung
- Holt-Oram-Syndrom
- Ventrikelseptumdefekt
- Eisenmenger-Reaktion
- Lutembacher syndrome
- erweiterte Pulmonalarterie
- Atriumseptumdefekt Ostium-Primum-Typ
- Atriumseptumdefekt Secundum-Typ
- sinus venosus atrial septal defect
und weiter:
- Lungenvenenfehlmündung
- Down-Syndrom
- Ebstein anomaly
- acyanotic congenital heart disease
- septal occluder
- Snowman heart
- Transposition der großen Arterien
- Roberts-Syndrom
- Varianten der Herzanatomie
- tricuspid atresia
- causes of pulmonary arterial hypertension
- Bland-White-Garland-Syndrom
- antenatal features of Down syndrome
- CXR approach to congenital heart disease
- Rubinstein-Taybi-Syndrom
- Thalidomid-Embryopathie
- partielle Lungenvenenfehlmündung
- Fetales Alkoholsyndrom
- paradoxical embolism
- chest x-ray appeoach to congenital heart disease
- Okkluder
- congenital heart disease - chest x-ray approach
- Thrombozytopenie-Radiusaplasie-Syndrom
- Raghib syndrome
- pentalogy of Fallot
- Cantrell’sche Pentalogie
- anomalous left coronary artery off the pulmonary artery
- Zyanotischer Herzfehler
- Vergrößerung rechter Ventrikel
- Vergrößerung rechter Vorhof
- Agenesie des Perikards
- differential of an enlarged pulmonary trunk on chest radiography
- Verschlusssystem Vorhofseptumdefekt
- Nicht-zyanotische Herzfehler
- Vorhofseptum
- Koronarsinusdefekt (unroofed coronary sinus)
- hypoplastic left heart syndrome with atrial septal defect
- preoperative evaluation of atrial septal defect using MRI
- akuter Verschluss der Arteria mesenterica superior


 Assoziationen und Differentialdiagnosen zu Atriumseptumdefekt:
Assoziationen und Differentialdiagnosen zu Atriumseptumdefekt: