calcium pyrophosphate deposition disease (CPPD)














 nicht verwechseln mit: Hydroxylapatit-Ablagerungserkrankung
nicht verwechseln mit: Hydroxylapatit-AblagerungserkrankungCalcium pyrophosphate dihydrate disease (CPPD), also known as pyrophosphate arthropathy or pseudogout, is defined by the co-occurrence of arthritis with evidence of CPPD deposition within the articular cartilage.
Terminology
The terminology regarding CPPD disease has been confusing, with chondrocalcinosis, CPPD, and pseudogout often used synonymously. Indeed, although initially described as chondrocalcinosis articularis, it is now understood that imaging findings of chondrocalcinosis do not always indicate CPPD disease .
In response, in 2011 the European League Against Rheumatism (EULAR) proposed a standardized terminology corresponding to clinical presentation :
- CPPD: occurrence of calcium pyrophosphate crystals, with or without symptoms
- asymptomatic CPPD: chondrocalcinosis +/- changes of osteoarthritis, but clinically asymptomatic
- acute CPPD crystal arthritis (formerly pseudogout): self-limiting synovitis in the setting of CPPD
- osteoarthritis with CPPD: typical changes of osteoarthritis in the setting of CPPD
- chronic CPPD crystal inflammatory arthritis
Epidemiology
CPPD is commonest in patients over the age of 50. Men and women are equally affected.
Clinical presentation
Most patients with imaging findings of CPPD are clinically asymptomatic.
Acute CPPD crystal arthritis (pseudogout) presents with severe acute or subacute pain, swelling, erythema, and warmth, of one or more joints and is usually self-limited. The presentation classically resembles an acute gout attack. Unlike gout, it most commonly involves the knee and the upper joints (shoulder, elbow, wrist). Another common joint is the pubic symphysis.
Chronic CPPD crystal inflammatory arthritis presents with chronic, intermittent painful swelling in the peripheral joints of upper and lower extremities.
Pathology
The crystals are weakly positively birefringent on polarized microscopy and have a rhomboid or rod shape.
Etiology
Causes of CPPD can be divided into:
- idiopathic
- hereditary
- AD pattern; mutation in the ANKH gene which encodes a transmembrane inorganic pyrophosphate transporter
- secondary
- hemochromatosis
- hyperparathyroidism
- hypothyroidism
- hypomagnesemia
- previous joint injury
- ochronosis
Radiographic features
CPPD has many features of osteoarthritis with an unusual distribution, for example, they tend to be symmetric in distribution and involve non-weight bearing joints or, in the hands, mainly involve the intercarpal and metacarpophalangeal joints.
Features of osteoarthritis in joints that are not commonly affected by it (i.e. non-weight bearing joints) :
- wrist joint (mainly radiocarpal and scapholunate joints)
- SLAC wrist can be seen in advanced cases
- a stepladder pattern of joint narrowing is classically described in which the narrowing is progressively less severe from the radiocarpal joint to the midcarpal joint
- metacarpophalangeal joints
- 2nd and 3rd preferentially
- hook-like osteophytes
- patellofemoral joint
- shoulder joint
- elbow joint
Chondrocalcinosis can occur in many locations. Notable sites include:
- knee: medial meniscus and patellofemoral joint
- wrist: triangular fibrocartilage complex and lunotriquetral ligaments
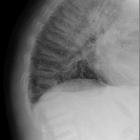
- pubic symphysis
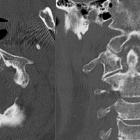
- spine
- chronic retro-odontoid pseudotumor
- crowned dens syndrome: acute pain and systemic inflammatory syndrome
- intervertebral discs
Large subchondral cysts may be present.
It is controversial whether gout leads to calcification of articular fibrocartilage or hyaline cartilage . CPPD disease can be differentiated from gout on ultrasound given that echogenic monosodium urate crystals line the surface of articular cartilage, whereas echogenic CPPD calcifications are located within the cartilage itself .
Differential diagnosis
Possible imaging differential considerations include
- osteoarthritis: usually have the typical weight-bearing distribution
- giant cell tumor (GCT): subchondral cysts of CPPD can be large and simulate subchondral GCT
See also
Siehe auch:
- Gicht
- Weichteilverkalkungen
- Arthrose
- Akromegalie
- primärer Hyperparathyreoidismus
- Morbus Wilson
- Hydroxylapatit-Ablagerungserkrankung
- Amyloidose
- Chondrokalzinose
- Hämochromatose
- Milwaukee-Schulter
- Ochronose
- chondrocalcinosis (mnemonic)
- Bursitis calcarea
- Hämophilie
- Denskrone
- Kristallarthropathie
- Keutel-Syndrom
- mnemonics
und weiter:
- Patellarsehnenruptur
- tumoröse Kalzinose
- subchondrale Zysten
- scapholunate advanced collapse (SLAC)
- radiologisches muskuloskelettales Curriculum
- Tendovaginitis
- Diskusverkalkungen
- ring- und bogenförmige Verkalkungen
- dens erosion
- temporomandibular joint inflammation
- subchondral cysts (mnemonic)
- calcium pyrophosphate dihydrate deposition arthropathy
- Chondrokalzinose Kniegelenk
- CPPD arthropathy wrist
- Arthritis der Schulter
- haemochromatosis - skeletal manifestations
- Alkaptonurie
- muskuloskelettale Manifestationen Hämochromatose
- Merkspruch Weichteilverkalkungen
- cppd spine
- cppd of the cervical spine


 Assoziationen und Differentialdiagnosen zu Kalziumpyrophosphat-Ablagerungskrankheit:
Assoziationen und Differentialdiagnosen zu Kalziumpyrophosphat-Ablagerungskrankheit: