immotile cilia syndrome





Primary ciliary dyskinesia, also known as immotile cilia syndrome, is the result of a congenital defect in the ultrastructure of cilia that renders them incapable of normal movement. It is associated with a number of anatomic and functional abnormalities.
Epidemiology
Primary ciliary dyskinesia is caused by a heterogeneous group of genetic abnormalities which are inherited in an autosomal recessive pattern. The incidence variably estimated at 1:12,000-60,000 .
Clinical presentation
As cilia are found in a number of locations both during the embryological period and extra-uterine life it is not surprising that a number of systems are involved. Most apparent is the involvement of the respiratory tract cilia and sperm. The clinical picture includes:
- chronic sinusitis and chronic otitis media:
- earliest clinical manifestation, as early as 6 months of age
- diagnosis is nonetheless often not suspected especially in the absence of situs inversus
- conductive hearing loss is common and may result in language delay
- bronchiectasis: main cause of morbidity
- impaired fertility
- sterility in males
- increased rate of ectopic pregnancy/subfertility in females
Additionally, normal ciliary function is believed to be responsible for normal lateralization of the asymmetric chest and abdominal organs. In patients with primary ciliary dyskinesia, there is a random orientation, with 50% of patients demonstrating situs inversus .
Diagnosis is confirmed by:
- beat analysis of cilia demonstrating abnormal, reduced, or absent ciliary motion
- electron microscopic ultrastructural analysis of respiratory cilia demonstrating the absence of, or abnormal dynein arms .
Two other tests are sometimes employed:
- saccharin test: time taken for sweet taste to be appreciated in the mouth, when a saccharin pellet is placed on the inferior turbinate, normal is less than 30 minutes
- nasal nitric oxide (nNO) measurement: typically very low (<250 ppb) in patients with PCD, CF, and severe rhinosinusitis
Pathology
A number of ciliary structural abnormalities are recognized, including :
- complete or partial absence of dynein arms: inner arms, outer arms or both
- radial spoke defect
- microtubular transposition
Irrespective of the specific defect, the result is abnormal ciliary movement, which manifest in a variety of epithelial surfaces (respiratory epithelium including that covering the middle ear, paranasal sinuses and pharynx), sperm tail movement and fallopian tube mucosa. The term 'immotile' may be a misnomer as some movement may be present, although it lacks coordination and strength .
Associations
A number of both syndromic and non-syndromic associations are recognized.
Syndromic
Various combinations of the above clinical features have been described as syndromes :
Non-syndromic
In addition, there may be an association with a number of other conditions, including:
- pectus excavatum
- hydrocephalus: thought due to abnormal ependymal cilia
- complex congenital heart disease
- biliary atresia
Radiographic features
Plain radiograph
Chest radiographic abnormalities are dominated by bronchial wall thickening, bronchiectasis and hyperinflation. In some instances, cystic bronchiectasis with air-fluid levels may be visible .
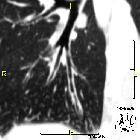
CT
The most striking pulmonary abnormality is that of bronchial wall thickening and bronchiectasis, present in most patients. The distribution is either central or diffuse and has a predilection for the lower and middle lobes .
CT sinuses
Evidence of chronic sinusitis is prominent and may be seen as early as 6 months of age. The middle ears are chronically opacified, and polyps are seen in approximately 20% of cases.
Treatment and prognosis
The natural progression of primary ciliary dyskinesia is relatively slow compared to cystic fibrosis for example, but nonetheless, up to 25% of patients eventually develop respiratory failure .
Treatment largely consists of physiotherapy, early treatment of chest infection and immunisation against influenza virus .
As is the case with cystic fibrosis there appears to be higher than expected infection rate with P. aeruginosa .
Complications
Relate predominantly to bronchiectasis and diffuse lung disease, and include:
- chronic pulmonary infection
- hemoptysis
Differential diagnosis
Consider other causes of bronchiectasis, including:
- cystic fibrosis (see below)
- Williams-Campbell syndrome
- allergic bronchopulmonary aspergillosis (ABPA)
- congenital tracheobronchomegaly (also known as Mounier Kuhn syndrome)
Cystic fibrosis and primary ciliary dyskinesia share a number of similarities including :
- both are hereditary with autosomal recessive inheritance
- both have sinus and lung disease
- both have infertility in males
Fortunately, a number of differences usually enable a clinical distinction to be made relatively easily :
- immotile cilia
- basically normal mucus, cilia cannot move normally
- normal ductus deferens, sperm cannot swim normally
- radiologic findings are much milder
- cystic fibrosis
- abnormal mucus, cilia cannot clear it
- normal sperm, ductus deferens is obliterated
- radiologic findings are more severe
Siehe auch:
- Bronchiektasen
- Allergische bronchopulmonale Aspergillose
- Alpha-1-Antitrypsin-Mangel
- Kartagener-Syndrom
- zystische Fibrose
- Williams-Campbell-Syndrom
- angeborene Tracheobronchomegalie
- Young syndrome
und weiter:


 Assoziationen und Differentialdiagnosen zu primäre ciliäre Dyskinesie:
Assoziationen und Differentialdiagnosen zu primäre ciliäre Dyskinesie:




