intestinal ischemia
































Mesenteric ischemia, also commonly referred to as bowel or intestinal ischemia, refers to vascular compromise of the bowel and its mesentery that in the acute setting has a very high mortality if not treated expediently. Mesenteric ischemia is far more commonly acute than chronic in etiology. This article is focused on acute mesenteric ischemia.
Clinical presentation
The presentation can vary with the underlying cause. Severe abdominal pain that is disproportionate to examination findings and that responds poorly to analgesia is a classic mode of presentation for acute mesenteric ischemia.
Pathology
Bowel ischemia severity ranges from mild (generally transient superficial changes of intestinal mucosa) to more dangerous and potentially life-threatening transmural bowel wall necrosis . If ischemia is severe enough and is not relieved quickly, then a predictable sequence of events will usually be observed:
Etiology
Mesenteric ischemia can be classified into broad groups according to etiology :
- acute mesenteric ischemia (95% cases)
- arterial occlusive mesenteric ischemia (60-85% cases)
- non-occlusive mesenteric ischemia (15-30% cases)
- veno-occlusive mesenteric ischemia (5-15% cases)
- mixed, e.g. strangulating bowel obstruction
- chronic mesenteric ischemia (5%)
Location
Sometimes it may be useful to think of mesenteric ischemia in the setting of location:
- small bowel ischemia
- large bowel ischemia (ischemic colitis)
Radiographic features
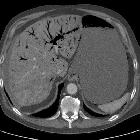
Although historically catheter angiography was the gold standard for imaging of suspected intestinal ischemia, CT has replaced it, with its ability to volumetrically assess the whole abdomen in multiple vascular phases, e.g. arterial, portal venous, delayed. It also has the added advantage of being able to diagnose alternative causes of acute abdominal pain. As such CT is now the investigation of choice for patients with suspected intestinal ischemia.
CT
Technique
In general CT of the abdomen and pelvis should be performed with intravenous contrast and a neutral luminal contrast (e.g. water) so that bowel wall enhancement and thickness can be adequately assessed . Ideally, positive oral contrast is best avoided to better delineate wall enhancement. Administration of positive rectal contrast may help define colonic wall thickening but is more useful when it is the distal colon which is affected (inferior mesenteric artery) - see ischemic colitis.
Multiple contrast phases are typically obtained:
Findings
Imaging features can vary depending on the time course and etiology and are therefore discussed separately in the articles above. A number of features are however common to most advanced acute cases and result from the bowel wall necrosis and perforation:
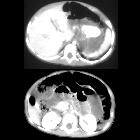
- pneumatosis intestinalis: gas in intestinal wall
- pneumatosis portalis: gas in the portal vein or in mesenteric vein
- can be differentiated by pneumobilia because gas usually reaches the periphery of the liver while pneumobilia is usually about 2 cm short of external liver border, and is more clustered at the hilum
- pneumoperitoneum: perforation of the bowel
- submucosal hemorrhage: sensitivity for diagnosis is low (10%) with all true-positive cases having other CT findings present at diagnosis
- variable amounts of free fluid
It is important to note that bowel wall thickness is not increased in all causes, and can in fact be thinned in complete arterial occlusion or bowel obstruction .
Dual-energy CT
The addition of iodine maps and 40-keV monoenergetic images to standard single energy CT images was found to increase reader confidence and accuracy in diagnosing acute bowel ischemia. Ischemic segments have been found to have lower densities and iodine concentrations compared to non-ischemic segments .
Treatment and prognosis
Although treatment will vary according to the severity and cause of the ischemia, in general treatment is surgical. The bowel needs to be assessed for viability and if necrotic needs to be resected. In some instances, endovascular thrombolysis/thrombectomy may be beneficial . Mortality rate is high at ~60% (range 30-90%) .
Siehe auch:
- Pneumoperitoneum
- Aerobilie
- Dünndarmileus
- Pneumatosis intestinalis
- Infarkt des Omentum majus
- Vaskulitis
- portalvenöses Gas
- Schockdarm
- Arteria mesenterica inferior
- Mesenterialvenenthrombose
- Dünndarmischämie
- intraperitonealer fokaler lipomatöser Infarkt
- ischämische Kolitis
- intramurale Gaseinschlüsse
- non occlusive mesenteric ischemia
- Dünndarmnekrose
- akuter Verschluss der Arteria mesenterica superior
- Verschluss der Arteria mesenterica superior
- acute radiation enteritis
- chronic radiation enteritis
- pneumatosis portalis
und weiter:
- Mesenterialinfarkt
- Volvulus
- Magenulkus
- closed loop obstruction
- Gas in Pfortader und Mesenterialvenen bei mesenterialem Infarkt
- Darmischämie
- CT Hypotensionskomplex
- Akutes Abdomen
- chronische mesenteriale Ischämie
- Viszeralarterien
- radiation enteritis
- Daumenabdruck-Zeichen
- pneumatosis intestinalis and hepatic portal venous gas
- Mesenteritis
- Ischämiezeichen Darm
- hämorrhagischer Dünndarminfarkt
- mesenteric ischaemia with intestinal necrosis
- Gas in der Ösophaguswand
- abdominelle Adhäsionen
- non occlusive mesenterial ischemia
- Einblutung in die Darmwand


 Assoziationen und Differentialdiagnosen zu Mesenterialinfarkt:
Assoziationen und Differentialdiagnosen zu Mesenterialinfarkt: