intrakranielles mykotisches (infiziertes) Aneurysma





Intracranial mycotic aneurysms, or intracranial infectious aneurysms, describe aneurysms arising from infection of the arterial wall of intracranial vessels.
See mycotic aneurysm for a general discussion on infectious aneurysms.
Epidemiology
The epidemiology of intracerebral mycotic aneurysms mirrors that of risk factors, the primary risk factor, accounting for nearly 70% of all cases, being left-sided infective endocarditis . In patients with infective endocarditis, up to 5% develop intracranial mycotic aneurysms . Up to 25% of affected patients have more than one intracerebral mycotic aneurysm .
Clinical presentation
Unruptured aneurysms present with non-specific clinical features, such as systemic symptoms (e.g. fever, weight loss), headache (localized or generalized), and transient focal neurological deficits from septic microemboli ; very rarely are intracerebral mycotic aneurysms large enough to cause signs and symptoms of mass-effect . Ruptured aneurysms present with clinical features of subarachnoid hemorrhage or intracerebral hemorrhage, such as meningism or stroke .
Pathology
Etiology
Intracerebral mycotic aneurysms are nearly always secondary to bacterial infection, however rarely fungal (e.g. neurocandidiasis, CNS aspergillosis) and viral etiologies (e.g. VZV, HIV-1) have been described . Viridans group Streptococcus (most common) and Staphylococcus aureus account for up to 90% of all intracranial mycotic aneurysms .
These aneurysms exist due to infection of the arterial wall . This generally occurs in the context of haematogenous spread from septic emboli to either the artery itself or its vasa vasorum, from which there is bacterial escape into the vessel wall, or in the context of direct bacterial extravascular invasion of the vessel wall . Direct extravascular invasion is rare and occurs in local pathologies (instead of infective endocarditis), such as meningitis, abscess, cavernous sinus thrombophlebitis, or orbital cellulitis .
Regardless of etiology, once bacteria are in the vessel wall, there is local arteritis resulting in degeneration of the elastic lamina and vessel wall . There is then subsequent formation of pseudoaneurysm through hydrostatic pulsations .
Location
Unlike berry aneurysms which are generally located at branch points of large circle of Willis vessels, bacterial intracerebral mycotic aneurysms have a predilection for more peripheral branch points (M2 and beyond), especially in the distal middle cerebral artery . However, up to one-third of all bacterial intracerebral mycotic aneurysms are proximally located, especially in cases of direct extravascular invasion .
In comparison, fungal intracerebral mycotic aneurysms tend to involve long segments of proximal larger circle of Willis vessels, often not involving branching points at all . Aneurysms may be larger and more rapidly growing in immunocompromised patients .
Radiographic features
Intracranial mycotic aneurysms can be evaluated with CT, MRI, or angiography .
Classically, the peripheral location of intracranial mycotic aneurysms allows them to be differentiated from berry aneurysms , however more proximal aneurysms can be impossible to differentiate from berry aneurysms on any imaging modality . Morphologically, these aneurysms are typically small , although rarely giant intracranial mycotic aneurysms have been described , and are typically fusiform (more common), saccular or sacculofusiform .
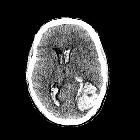
CT
CT is often utilized as a first-line imaging modality given its accessibility . Non-contrast studies may show complications of the aneurysm, such as subarachnoid hemorrhage (often convexal), intracerebral hemorrhage (often lobar), abscess, or ischemic stroke, while the aneurysm may be identified with CT angiography .
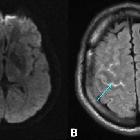
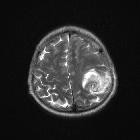
MRI
MRI has a similar utility to that of CT, however is considered to be slightly more sensitive . Advantages include use of susceptibility-sensitive sequences, such as GRE or SWI, which may reveal evidence of subclinical or asymptomatic bleeding (e.g. microbleeds, cortical superficial siderosis) from ruptured aneurysms, and use of DWI which may show subclinical or asymptomatic ischemic strokes not visible on CT .
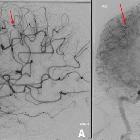
DSA
Digital subtraction angiography is considered the gold-standard imaging modality for the evaluation of intracranial mycotic aneurysms . In particular, DSA is the most reliable imaging modality for detecting small aneurysms (<3 mm in size) .
Treatment and prognosis
In addition to management of underlying source of infection, two approaches may be taken :
- antibiotics alone (conservative approach)
- antiobiotics combined with a surgical approach
A conservative management approach with antibiotics alone is reserved for cases of unruptured intracranial mycotic aneurysms or in patients not suitable for surgical approaches . Varying success has been reported using this strategy, with studies consistently finding ~30% of aneurysms disappear, ~20% decrease in size, 15-30% have no significant change in size, and ~20% actually increase in size . Thus, while this may be an effective approach, serial angiographic follow-up is required to assess efficacy of therapy on aneurysm size .
Management with antibiotics and surgery is an option for both unruptured and ruptured intracranial mycotic aneurysms . Surgical options include clipping, which was traditionally the favored approach, or novel endovascular approaches (e.g. endovascular coil embolization), which are gathering more evidence in recent literature . In recent comparisons, the two surgical techniques have similar outcomes .
Even with management, prognosis is poor; unruptured intracranial mycotic aneurysms have a mortality of up to 30%, while ruptured intracranial mycotic aneurysms have a mortality of up to 80% . Outcomes are poorer for patients with multiple intracerebral mycotic aneurysms .
History and etymology
Intracranial mycotic aneurysms were first described by W S Church, an English physician, in 1869 , with coinage of the term 'mycotic aneurysm' provided by Sir William Osler (1849-1919), a Canadian physician, in 1885 . During this period, 'mycotic' was used to describe all micro-organisms, and thus 'mycotic aneurysm' described any infectious aneurysm - a term which has persisted in medical literature .
Differential diagnosis
See also
Siehe auch:


 Assoziationen und Differentialdiagnosen zu intrakranielles mykotisches (infiziertes) Aneurysma:
Assoziationen und Differentialdiagnosen zu intrakranielles mykotisches (infiziertes) Aneurysma:
