non-ossifying fibroma















































Non-ossifying fibromas (NOF) are the most common type of non-neoplastic fibrous bone lesionand are a larger version (>3 cm) of a fibrous cortical defect; both are encompassed by the term fibroxanthoma or metaphyseal fibrous defect.
Epidemiology
Non-ossifying fibromas are very common in children and adolescents, and the most common fibrous, bony lesion in this age group , with a peak incidence at 10-15 years of age. The prevalence is estimated at 30-40% of all normal children. It is twice as common in boys than in girls . They are usually not seen beyond the age of 30, as they spontaneously heal, being gradually filled in by bone.
Clinical presentation
The majority of non-ossifying fibromas are asymptomatic. Larger lesions may be painful and potentially weaken the bone enough to predispose to pathological fracture.
Multiple non-ossifying fibromas are associated with neurofibromatosis type 1 (NF1) and Jaffe-Campanacci syndrome.
Rarely fibroxanthomas can cause hypophosphatemic vitamin D-resistant rickets .
Pathology
A non-ossifying fibroma appears macroscopically as a fleshy, fibrous, yellow or tan-brown lesion with variable areas of hemorrhage .
Microscopic examination reveals the lesions to be highly cellular containing spindle-shaped cells on a background of stromal tissue in a prominent storiform pattern. Foamy histiocytes and multinucleated giant cells are also seen. Mitotic figures and/or cellular dysplasia should not be seen .
The irony of non-ossifying fibromas appearing to ossify has not been lost on generations of radiologists, although strictly speaking the lesion itself does not ossify, rather being filled in by normal bone from the periphery . Indeed, it is believed that many bone islands are healed fibroxanthomas (FCD/NOF).
Radiographic features
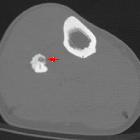
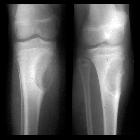
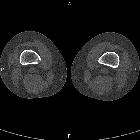
Plain radiograph / CT
Non-ossifying fibromas are typically a multiloculated lucent lesion with a sclerotic rim. They are located eccentrically in the metaphysis, adjacent to the physis. As the patient ages, they seem to migrate away from the physis .
They have no associated periosteal reaction, cortical breach or associated soft tissue mass.
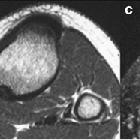
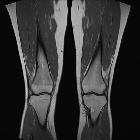
MRI
MRI appearances of non-ossifying fibromas are variable and depend on when along with the development and healing phase the lesion is imaged.
Initially, the lesion has a high or intermediate T2 signal, with a peripheral low signal rim corresponding to the sclerotic border. As it matures and begins to ossify, the signal becomes low on all sequences .
Contrast enhancement is also variable .
Nuclear medicine
Appearance on bone scan depends on the phase of the lesion:
- non-ossifying fibromas are usually not associated with increased activity
- mild to moderately increased activity can be seen during non-ossifying fibroma "healing", corresponding to mild hyperemia and osteoblastic activity
- note that extensive uptake or hyperemia should prompt consideration of alternative diagnosis or a superimposed fracture
Treatment and prognosis
Non-ossifying fibroma is one of the skeletal “Don’t touch” lesions.
Most non-ossifying fibromas require no treatment or biopsy. If large (involving more than 50% of the diameter of the parent bone) then prophylactic curettage and bone grafting may be prudent to avoid a pathological fracture .
Differential diagnosis
General imaging differential considerations include:
- fibrous cortical defect
- aneurysmal bone cyst (ABC)
- eccentric lytic metaphyseal lesion
- MRI differentiates ABC by fluid-fluid levels
- chondromyxoid fibroma
- fibrous dysplasia
- desmoplastic fibroma
- Langerhans cell histiocytosis
See also
Siehe auch:
- Osteoid-Osteom
- Fibröse Dysplasie
- Aneurysmatische Knochenzyste
- Stressfraktur
- kortikales Desmoid
- Ossifizierendes Fibrom
- Chondromyxoidfibrom
- desmoplastisches Fibrom
- Fokale kortikale Dysplasie
- ausgeheiltes nicht ossifizierendes Fibrom (NOF)
- fibröser Kortikalisdefekt
- lytic bone lesion (mnemonic)
- Fibroxanthom des Knochens
- fokale fibrokartilaginäre Dysplasie
- Fibroxanthom
- nicht ossifizierendes Fibrom der Tibia
und weiter:
- intraossäres Ganglion
- einfache (juvenile) Knochenzyste
- Knocheninfarkt
- Riesenzelltumor
- solide Periostreaktion
- Jaffé-Campanacci-Syndrom
- Riesenzelltumor des Knochens
- nicht ossifizierendes Fibrom distales Femur
- diaphyseal lesions (mnemonic)
- benignes fibröses Histiozytom des Knochens
- Ostitis fibrosa cystica
- Osteoklastom
- focal sclerotic bony lesions (mnemonic)
- fibrous lesions
- Dermatofibrom
- Riesenzelltumor des Beckenknochens
- skelettale "do not touch"-Läsionen
- focal fibrocartilaginous dysplasia of the tibia
- polyostotic bone lesions in adults
- Knochenläsionen der Metaphyse
- FCD
- lytic lesion of the femur in children
- bony lesions without periostitis or pain (mnemonic)
- neurofibromatosis I affecting long bones
- multifocal non-ossifying fibroma in the lower limbs


 Assoziationen und Differentialdiagnosen zu nicht ossifizierendes Fibrom:
Assoziationen und Differentialdiagnosen zu nicht ossifizierendes Fibrom: