dural sinus thrombosis
























































Dural venous sinus thrombosis (plural: thromboses) is a subset of cerebral venous thrombosis, often coexisting with cortical or deep vein thrombosis, and presenting in similar fashions, depending mainly on which sinus is involved.
As such, please refer to the cerebral venous thrombosis article for a general discussion.
Epidemiology
Any age women on the contraceptive pill are over-represented. Please refer to the article on cerebral venous thrombosis for a broad discussion on epidemiology and risk factors.
Clinical presentation
Presentation is variable and can range from asymptomatic to coma and death. Typically patients complain of headache, nausea, and vomiting. Neurological deficits are variable.
Pathology
Superior sagittal sinus or the dominant transverse sinus thrombosis can affect the arachnoid granulation absorption of cerebrospinal fluid; consequent cerebral swelling may occur . The subsequent venous hypertension can lead to edema and hemorrhage.
Risk factors
- hormonal
- oral contraceptive pill, pregnancy, puerperium, steroids, hyperthyroidism
- prothrombotic hematological conditions
- protein S deficiency, polycythemia
- local factors
- skull abnormalities, infections (especially mastoid sinus - dural sinus occlusive disease), head injury (especially skull fractures that extends to a dural venous sinus)
- systemic illness
- dehydration, sepsis, malignancy, connective tissue disorders
- idiopathic: ~12.5%
Please refer to the generic article for a broad discussion on pathology: cerebral venous thrombosis.
Radiographic features
Any of the dural sinuses can be affected, in isolation or combined/continuous with one another:
- superior sagittal sinus thrombosis
- straight sinus thrombosis
- transverse sinus thrombosis
- sigmoid sinus thrombosis (including dural sinus occlusive disease (DSOD)
- cavernous sinus thrombosis
CT
Unenhanced CT is usually the first imaging investigation performed given the nonspecific clinical presentation in these cases. When not associated with venous hemorrhage or infarction, it can be a subtle finding on CT images, relying on hyperdensity of the sinus being identified. Potential findings include:
- cord sign
- dense vein sign
- a potential pitfall is interpreting the distal superior sagittal sinus as being hyperdense near the torcula herophili; it is important to appreciate that normal blood within the dural sinuses is usually of slightly increased density relative to brain parenchyma and that true hyperdensity is the key to recognizing thrombosis
- The walls at this location can be thick, measuring up to 2-3 mm
- cerebral/cortical edema: secondary to venous hypertension
- unilateral or bilateral cortical or peripheral venous hemorrhage
With contrast administration, especially with a CT venogram, a sinus filling defect is sought. Multiplanar reformatted CT venography has been reported with a sensitivity of 95% for this diagnosis. Signs on contrast CT include:
- empty delta sign (specific to a superior sagittal sinus thrombosis)
- gyral enhancement
- prominent intramedullary vein
Caution must be taken to achieve a well-timed acquisition in CT cerebral venography, particularly in cases of intracranial hypertension which can cause delayed filling of the venous sinus. A premature acquisition may create a false impression of thrombosis, which is simply due to contrast not yet reaching the venous sinuses - if the cerebral veins are not opacified on a CT cerebral venogram, premature acquisition should be suspected.
In the blunt head trauma setting, there are findings that correlate with an increased risk of dural venous sinus thrombosis and thereby promote CT venogram confirmation:
- skull fractures that extend to a dural venous sinus
- skull base fractures that involve the groove for the sigmoid sinus
- dural sinus hyperdensity
- intrasinus gas
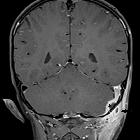
MRI
MRI is able to both visualize the clot as well as the sequelae.
Conventional spin-echo sequences may demonstrate an absence of normal flow void on the dural sinuses. The clot acutely is isointense on T1 and hypointense on T2 (this can mimic a flow void), with subacute clot becoming hyperintense on T1. All the findings listed in the CT section are also seen on MRI. The most sensitive conventional MRI sequence for detection of the clot is susceptibility sequences such as SWI or GRE. Overall, the conventional MRI sequences in combination are very sensitive but relatively non-specific in the detection of dural venous sinus thromboses. Contrast-enhanced 3D T1WI GRE is the most sensitive and specific MRI sequence in the detection of DVST; MRV will demonstrate a lack of flow.
Staging severity
Dural venous thromboses can result in parenchymal edema and ischemia in its watershed area; the severity of which can be graded as follows:
- type 1: no imaging abnormality
- type 2: high T2
- type 3: high T2 with enhancement
- type 4: hemorrhage or infarction
Treatment and prognosis
Systemic anticoagulation (e.g. heparin and warfarin) is still the first-line treatment for dural venous thrombosis. Anticoagulation is usually required even in the setting of venous hemorrhage.
Interventional management includes microcatheter thrombolysis or thromboplasty.
Dural arteriovenous fistula and increased CSF pressure have been reported as possible complications after dural venous sinus thrombosis.
For a general discussion on treatment please refer to the parent article: cerebral venous thrombosis.
Differential diagnosis
- asymmetric anatomy: hypoplasia or atresia of the transverse sinus
- the right transverse sinus is larger than the left in most patients
- if the sinus is small or absent, then the ipsilateral sigmoid sinus and jugular fossa should also be small
- arachnoid granulations:
- usually characterized as well-defined focal filling defects within the dural venous sinuses (measuring 2–9 mm in diameter)
- these are more common in the lateral aspects of the transverse sinuses and should follow CSF signal intensity on all MRI sequences
- asymmetric flow in the transverse or sigmoid sinus can mimic a dural venous thrombosis
Practical points
- infarction in a non-arterial location, especially when bilateral or hemorrhagic
- cortical or peripheral hemorrhage, especially when heterogeneous and gyriform
- cortical edema
- direct signs of a thrombus (e.g. dense clot sign, cord sign, empty delta sign)
- anatomy variations commonly occur and can mimic sinus thrombosis or occlusion
Siehe auch:
- Pacchionische Granulationen
- Sinus durae matris
- empty delta sign
- oberflächliche Venenthrombose
- zerebrale Venenthrombose
- tiefe Venenthrombose
- Sinusthrombose bei otogenen Infektionen
- venöser zerebraler Infarkt
- cerebral venous infarct secondary to venous sinus thrombosis
- Lillie-Crowe sign
- cord sign
- Sinus cavernosus Thrombose
- Thalamusblutung
- Pacchionische Granulationen in den duralen venösen Sinus
- Fett in den intrakranialen venösen Sinus
- Sinusthrombose Sinus sagittalis superior
- Herniation von Hirngewebe in durale Sinus
- Virchow`s triad
- durale venöse Sinuszysten (DVSZ)
und weiter:
- Developmental Venous Anomaly
- Tentorium cerebelli
- Hirnabszess
- Sinus transversus
- Meningitis
- neuroradiologisches Curriculum
- Idiopathische intrakranielle Hypertension
- Orbitaphlegmone
- akute Sinusitis
- Gradenigo-Syndrom
- Hughes-Stovin-Syndrom
- Venae emissariae
- inferior petrosal sinus sampling
- oberflächliche anastomosierende Venen des humanen Cortex
- superficial cerebral vein thrombosis
- venous thromboembolism
- Antiphospholipid-Syndrom
- Thrombose der tiefen Hirnvenen
- Pyramidenspitzen-Osteomyelitis
- lateral lacunae of superior sagittal sinus
- sinus sagittalis lesion
- tuberkulöse Otomastoiditis
- Kontrastmittelaussparung venöse Sinus
- pregnancy related sinus thrombosis with venous infarction
- einschmelzende Mastoiditis mit Sinusthrombose
- sagittal sinus thrombosis
- Lipome in den intrakranialen venösen Sinus
- superior sagittal sinus thrombosis on ADC maps of diffusion MRI
- postthrombotic sinus sagittalis


 Assoziationen und Differentialdiagnosen zu Sinusthrombose:
Assoziationen und Differentialdiagnosen zu Sinusthrombose:







