Aortendissektion bei Aortenisthmusstenose










Aortendissektion bei Aortenisthmusstenose
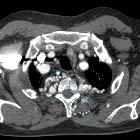
Aortendissektion Radiopaedia • CC-by-nc-sa 3.0 • de
Aortic dissection is the most common form of the acute aortic syndromes and a type of arterial dissection. It occurs when blood enters the medial layer of the aortic wall through a tear or penetrating ulcer in the intima and tracks along the media, forming a second blood-filled channel within the wall.
Epidemiology
The majority of aortic dissections are seen in elderly hypertensive patients. In a very small minority, an underlying connective tissue disorder may be present. Other conditions or predisposing factors may also be encountered, in which case they will be reflected in the demographics. Examples include :
- structural aortic abnormalities
- bicuspid aortic valve
- aortic coarctation
- abnormal connective tissues
- Turner syndrome
- pregnancy
- intra-aortic balloon pumps
- ciprofloxacin use (unclear if class effect for fluoroquinolone agents)
- fluoroquinolones seem to promote loss of extracellular matrix integrity, by several mechanisms
- in the UK caution is now advised in using these agents in high-risk patients
Clinical presentation
The duration of aortic dissection is arbitrarily categorised into three phases :
- acute: within 14 days of first symptom onset
- subacute: between 14 days to 3 months
- chronic: more than 3 months from the initial onset of symptoms
Patients are often hypertensive (although they may be normotensive or hypotensive) and present with anterior or posterior chest pain and a tearing sensation in the chest. There may be a difference in blood pressure between the two arms depending on where the dissection occurs.
Depending on the extent of dissection and occlusion of aortic branches, end-organ ischaemia may also be present (seen in up to 27% of cases) , including:
- abdominal organ ischaemia
- limb ischaemia
- ischaemic or embolic stroke
- paraplegia: involvement of the artery of Adamkiewicz
If the aortic dissection involves the aortic root it may result in involvement of the coronary arteries and can present similarly to ST-elevation myocardial infarction on an ECG. However, treating these patients with antiplatelets/anticoagulation could be disastrous in aortic dissection.
Some cases of aortic dissection may result in rupture, causing collapse and often death. Signs of cardiac tamponade (Beck's triad) may also be encountered if rupture occurs into the pericardial space.
There have been efforts to construct a clinical decision rule stratify risk of acute aortic dissection and avoid over-investigation. The aortic dissection detection risk score (ADD-RS) combined with a negative D-dimer test has been demonstrated to be effective in reducing unnecessary exams, however, it has not been widely accepted into clinical practice and requires further validation .
Pathology
The normal lumen lined by intima is called the true lumen and the blood-filled channel in the media is called the false lumen. In most cases the vessel wall is abnormal. Causes include:
- hypertension (pathogenesis: medial degeneration)
- inherited connective tissue disorders (pathogenesis: medial degeneration)
- atherosclerosis (pathogenesis: penetrating ulcer)
- vasculitis (pathogenesis: inflammation)
- pregnancy (pathogenesis: unknown)
- iatrogenic: aortic catheterisation, intra-aortic balloon pump
Radiographic features
Imaging is essential in delineating the morphology and extent of the dissection as well as allowing for classification (which dictates management). Two classification systems are in common usage, both of which divide dissections according to the involvement of the ascending aorta:
In recent years, the Stanford classification has gained favour with cardiothoracic surgeons. Approximately 60% of dissections involve the ascending aorta (Stanford A or DeBakey I and II) .
Aortic dissection is may sometimes be classified as communicating versus non-communicating .
A new classification system was proposed which is referred with the acronym DISSECT (duration, intimal tear, size of the dissected aorta, the segmental extent of involvement, clinical complications, and thrombosis of the false lumen).
Plain radiograph
Chest radiography may be normal or demonstrate a number of suggestive findings, including:
- widened mediastinum: > 8.0-8.8 cm at the level of the aortic knob on portable anteroposterior chest radiographs , although this upper limit of normal varies (may be significantly larger) depending on projection, FFD and x-ray cassette positioning
- double aortic contour
- irregular aortic contour
- inward displacement of atherosclerotic calcification (>1 cm from the aortic margin)
Depending on aetiology, there may be signs of periaortic or mediastinal haematoma which include:
- obscuration of the aortic knob
- opacification of the AP window
- deviation of mediastinal structures
- oesophagus or NGT to the right
- trachea to the right
- left main bronchus inferiorly (decreased angle from the horizontal)
- increased thickness of the left and/or right paratracheal stripe
- apical capping, particularly on the left
CT
CT, especially with arterial contrast enhancement (CTA) is the investigation of choice, able not only to diagnose and classify the dissection but also to evaluate for distal complications. It has reported sensitivity and specificity of nearly 100% .
Non-contrast CT may demonstrate only subtle findings; however, a high-density mural haematoma is often visible. Displacement of atherosclerotic calcification into the lumen is also a frequently identified finding.
Dissections involving the aortic root should ideally be assessed with ECG-gated CTA which nearly totally eliminates pulsation artefact. Pulsation artefact can mimic dissection, is very common and seen in up to 92% of non-gated CTA studies .
Contrast-enhanced CT (preferably CTA) gives excellent detail. Findings include :
- intimal flap
- double-lumen
- dilatation of the aorta
- complications (see below)
- an atypical variant that may be seen is an aortic intramural haematoma
- Mercedes-Benz sign in the case of a "triple-barreled" dissection
- windsock sign
The CTA-report should include at least:
- proximal and distal extent of dissection
- location of the intimal tear
- aortic size
- involvement and supply (from true or false lumen) of aortic branches
- signs of organ ischaemia or vessel occlusion
An essential part of the assessment of aortic dissection is identifying the true lumen, as the placement of an endoluminal stent-graft in the false lumen can have dire consequences. Distinguishing between the two is often straightforward, but in some instances, no clear continuation of one lumen with normal artery can be identified. In such instances, a number of features are helpful :
- true lumen
- often compressed by the false lumen and the smaller of the two
- outer wall calcifications (helpful in acute dissections)
- origin of the coeliac trunk, SMA and right renal artery usually arise from the true lumen
- false lumen
- often larger lumen size due to higher false luminal pressures
- at risk for rupture due to reduced elastic recoil and dilation
- beak sign
- cobweb sign (as slender linear areas of low attenuation specific to the false lumen due to residual ribbons of media that have incompletely sheared away during the dissection process)
- often of lower contrast density due to delayed opacification
- maybe thrombosed and seen as mural low density only (more common in chronic dissections)
- the left renal artery usually arises from the false lumen
- surrounds true lumen in Stanford type A
Chronic dissection flaps are often thicker and straighter than those seen in acute dissections .
Transoesophageal echocardiography
Transoesophageal echocardiography (TOE) has very high sensitivity and specificity for assessment of acute aortic dissection, but due to limited access and its invasive nature, it has largely been replaced by CTA (or MRA in some instances) .
MRI
Although in general MRA has been reserved for follow-up examinations, rapid non-contrast imaging techniques (e.g. true FISP) may see MRI having a larger role to play in the acute diagnosis, particularly in patients with impaired renal function . It has similar sensitivity and specificity to CTA and TOE but suffers from limited availability and the difficulties inherent in performing MRI on acutely unwell patients.
DSA - angiography
Conventional digital subtraction angiography has historically been the gold standard investigation. CTA has now replaced it as the first-line investigation, not only due to it being non-invasive but also on account of better delineation of the poorly opacifying false lumen, intramural haematoma and end-organ ischaemia.
Angiography still is required for endoluminal repair.
Risks of angiography include general risks of angiography plus the risk of catheterising the false lumen and causing aortic rupture.
Treatment and prognosis
- aggressive blood pressure control with beta-blockers as they reduce both blood pressure and also heart rate hence reduce extra pressure on the aortic wall
- immediate surgical repair (for type A dissection or complicated type B dissection)
Complications
Complications of all types of aortic dissection include:
- dissection and occlusion of branch vessels
- abdominal organ ischaemia
- limb ischaemia
- ischaemic stroke
- paraplegia: involvement of artery of Adamkiewicz
- distal thromboembolism
- aneurysmal dilatation: this is an indication for endovascular or surgical intervention
- aortic rupture
A Stanford type A dissection may also result in:
- coronary artery occlusion
- aortic incompetence
- rupture into the pericardial sac with resulting cardiac tamponade
Although the combination of blood pressure control and surgical intervention has significantly lowered in-hospital mortality, it remains significant, at 10-35%. Over the 10 years following diagnosis another 15-30% of patients require surgery for life-threatening complications .
Differential diagnosis
The differential on chest x-ray is that of a dilated thoracic aorta.
On CT, a number of entities that can mimic a dissection should be considered :
- pseudodissection due to aortic pulsation motion artefact (typically left anterior and right posterior aspects of the ascending aorta)
- pseudodissection due to contrast streaks
- mural thrombus
- intramural haematoma: really an atypical type of aortic dissection and part of the acute aortic syndrome
- penetrating atherosclerotic ulcer which is part of the acute aortic syndrome
- adjacent atelectasis
- minimal aortic injury
Clinically, a number of causes of acute chest pain are often considered:
- acute coronary syndrome
- acute pulmonary embolism
- pneumonia
- Bornholm disease: a diagnosis of exclusion, rarely thought about. CT usually normal, or occasionally non-specific pleural inflammation and/or infiltrates.
Aortenisthmusstenose Radiopaedia • CC-by-nc-sa 3.0 • de
Coarctation of the aorta (CoA) refers to a narrowing of the aortic lumen.
Epidemiology
Coarctations account for between 5-8% of all congenital heart defects. They are more frequent in males, M:F ratio of ~2-3:1.
Clinical presentation
Varies accordingly to the degree of stenosis and the associated abnormalities. Patients may be asymptomatic in a setting of non-severe stenosis.
Children and adults can present with angina pectoris and leg claudication. On clinical examination, diminished femoral pulses and differential blood pressure between upper and lower extremities may be noted.
ECG
- high left ventricular voltage (HLVV)
- voltage criteria present for left ventricular hypertrophy
- left ventricular "strain" pattern
- variably present in the lateral leads (I, aVL, V5-6)
- asymmetric T-wave inversion originating from a depressed ST segment
- right ventricular hypertrophy
- less common
Pathology
It can be primarily divided into two types:
- characterized by diffuse hypoplasia or narrowing of the aorta from just distal to the brachiocephalic artery to the level of ductus arteriosus
- typically with a more discrete area of constriction just proximal to the ductus but distal to the origin of the left subclavian artery
- therefore, the blood supply to the descending aorta is via the patent ductus arteriosus
- characterized by a short segment abrupt stenosis of the post-ductal aorta
- it is due to thickening of the aortic media and typically occurs just distal to the ligamentum arteriosum (a remnant of the ductus arteriosus)
Associations
As with many congenital abnormalities, coarctation of the aorta is associated with other congenital anomalies.
- cardiac
- bicuspid aortic valve: most common associated defect and seen in 75-80%
- ventricular septal defect
- cyanotic congenital lesions including
- truncus arteriosus
- transposition of the great arteries, especially with a sub-pulmonic VSD and overriding pulmonary artery (Taussig-Bing)
- mitral valve defects including
- hypoplastic mitral valve
- parachute mitral valve
- abnormal papillary muscles
- patent ductus arteriosus
- non cardiac
- intracranial berry aneurysms
- spinal scoliosis
- syndromic associations
- cardiac
- wider syndromic
- PHACE syndrome
- Turner syndrome: a coarctation can be seen in 15-20% of those with Turner syndrome
Radiographic features
Plain radiograph
- figure of 3 sign: contour abnormality of the aorta
- inferior rib notching: Roesler sign
- secondary to dilated intercostal collateral vessels which form as a way to bypass the coarctation and supply the descending aorta
- the dilated and tortuous vessels erode the inferior margins of the ribs, resulting in notching
- seen only in long standing cases, and therefore not seen in infancy (unusual in patients <5 years of age)
- seen in 70% of cases presenting in older children or adults
- if the coarctation is distal to either subclavian artery, then increased flow occurs through the subclavian artery, forming a collateral pathway via the internal thoracic artery, anterior intercostal artery, posterior intercostal artery and then into the descending thoracic aorta
- usually the 4 to 8 ribs are involved; occasionally involves the 3rd to 9th ribs
- as the 1st and 2nd posterior intercostal arteries arise from the costocervical trunk (a branch of the subclavian artery) and do not communicate with the aorta, these are not involved in collateral formation, and the 1st and 2nd ribs do not become notched
- if bilateral rib notching: the coarctation must be distal to the origin of both subclavian arteries, to enable bilateral collaterals to form
- if unilateral right rib notching
- then the coarctation lies distal to the brachiocephalic trunk but proximal to the origin of the left subclavian artery
- or there may be a right sided aortic arch with aberrant left subclavian artery distal to coarctation
- collaterals cannot form on the left, as the left subclavian is distal to the coarctation
- if unilateral left rib notching, then this suggests an associated aberrant right subclavian artery arising after the coarctation
- the coarctation is distal to the origin of the left subclavian artery, therefore collaterals form on the left
- collaterals cannot form on the right, as the aberrant right subclavian artery arises after the coarctation
Antenatal ultrasound
Useful in assessing for infantile coarctations. The suprasternal notch-long axis views are considered helpful. The fetal right ventricle can be appear enlarged in severe coarctations although this alone is not a specific feature. Occasionally an aortic arch view may directly show a narrowing.
Echocardiography
Best visualized from the suprasternal window with transthoracic echocardiography and the upper esophageal positions with a transesophageal approach. Features commonly present include :
- reduction in luminal caliber of the descending aorta
- often accompanied by post-stenotic dilatation
- demonstrates sudden increase in velocity as measured by pulsed wave Doppler
- the continuous wave Doppler envelope will demonstrate the characteristic "shark tooth" morphology
- sharply elevated systolic peak
- diastolic velocity profile markedly concave
- the continuous wave Doppler envelope will demonstrate the characteristic "shark tooth" morphology
- left ventricular hypertrophy
Angiography: CTA/MRA/DSA
All modalities are capable of delineating the coarctation as well as collateral vessels, most common collateral pathway being subclavian artery to internal mammary artery to intercostal arteries (resulting in inferior rib notching) to post-coarctation part of descending thoracic aorta.
Treatment and prognosis
The urgency of treatment depends on the presence of congestive cardiac failure. This is usually the case in severe coarctations found in infancy. In less severe cases, elective treatment when the child is older (typically ~2 years of age) is preferred .
Treatment can be either primary surgical repair with excision of the coarctation and end-to-end anastomosis, or balloon angioplasty. Subclavian flap repair is a common surgical technique used, where the origin and proximal left subclavian artery is excised, opened up and sutured onto the aorta. If the subclavian is ligated, it is usually anastomosed onto the left common carotid artery.
Complications
- neonatal heart failure
- subarachnoid hemorrhage from a ruptured berry aneurysm
- aortic dissection
- infective endocarditis: in the context of an added infective insult
- mycotic aneurysm: in the context of an added infective insult
Differential diagnosis
Imaging differential considerations include:
- pseudo-coarctation of the aorta: elongation, narrowing or kinking with no pressure gradient or collateral formation, no rib notching
- chronic large vessel arteritis, e.g. chronic phase of Takayasu arteritis


 Assoziationen und Differentialdiagnosen zu Aortendissektion bei Aortenisthmusstenose:
Assoziationen und Differentialdiagnosen zu Aortendissektion bei Aortenisthmusstenose:
