intraventrikuläre Blutung



















Intraventricular hemorrhage denotes the presence of blood within the cerebral ventricular system. It is associated with significant morbidity due to the risk of obstructive hydrocephalus.
It can be divided into primary or secondary, primary hemorrhage being far less common than secondary:
- primary: blood in the ventricles with little (if any) parenchymal blood
- secondary: a large extraventricular component is present (e.g. parenchymal or subarachnoid) with secondary extension into the ventricles
In adults, secondary intraventricular hemorrhage is usually the result of an intracerebral hemorrhage (typically basal ganglia hypertensive hemorrhage) or subarachnoid hemorrhage with ventricular reflux.
Intraventricular hemorrhage is a distinct entity in pediatrics and considered separately; see intraventricular hemorrhage of the newborn.
Epidemiology
There are numerous causes of intraventricular hemorrhage and as such no single demographic can be identified; rather each underlying etiology contributes its own patient population. Having said that, secondary hemorrhage is far more common and as such the dominant demographic is that of patients with intraparenchymal or subarachnoid hemorrhage: older individuals are thus most commonly affected.
Clinical presentation
Clinical presentation of intraventricular hemorrhage (regardless of cause) is similar to that of subarachnoid hemorrhage. Patients experience sudden onset of severe headache . Signs of meningism are also present (i.e. photophobia, nausea and vomiting and neck stiffness). Larger hemorrhages can result in loss of consciousness, seizures, and brainstem compression with cardiorespiratory compromise.
Pathology
Etiology
Secondary intraventricular hemorrhage is much more common than primary IVH .
Primary
Some of the more common causes of primary intraventricular hemorrhage in adults include :
- hypertension
- vascular malformations
- aneurysm (e.g. PICA aneurysms have a tendency to fill the 4th ventricle, with little basal cistern blood)
- arteriovenous malformations (AVM)
- subependymal cavernous malformations
- anticoagulation therapy/coagulopathy
- intraventricular tumors
- ependymoma
- choroid plexus / intraventricular metastases
- adjacent parenchymal tumors (e.g. glioblastoma)
Secondary
Secondary causes of intraventricular hemorrhage include:
- extension from other intracerebral hemorrhages
- hypertensive hemorrhage, especially basal ganglia hemorrhage (common)
- lobar hemorrhage
- subarachnoid hemorrhage
- trauma
Radiographic features
CT
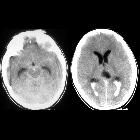
Non contrast CT of the brain is the mainstay of acute evaluation of patients presenting with sudden onset headache or stroke-like symptoms. Blood in the ventricles appears as hyperdense material, heavier than CSF and thus tends to pool dependently, best seen in the occipital horns. Acutely, if the volume is significant blood can fill the ventricle, and clot forming a 'cast'.
There is often obstructive hydrocephalus, and care must be taken in distinguishing this from ex vacuo dilatation of the ventricles.
MRI
MRI is more sensitive than CT to very small amounts of blood, especially in the posterior fossa, where CT remains marred by artifact.
Both FLAIR and more recently SWI (especially at 3T) are sensitive to small amounts of blood. Especially the latter will demonstrate tiny amounts of blood pooling in the occipital horns, and resulting in susceptibility induced signal drop out .
On FLAIR the signal intensity will vary depending on the timing of the scan. Within 48 hours blood will appear as hyperintense to the attenuated adjacent CSF . Later the signal is more variable and can be difficult to distinguish from flow related artifact (particularly in the third and fourth ventricles) unless other sequences are also used.
Treatment and prognosis
The main treatment approaches of intraventricular hemorrhage can be divided into two:
- treatment of the underlying cause of hemorrhage (e.g. aneurysm, AVM)
- treatment of obstructive hydrocephalus
The latter may merely require careful monitoring of clinical state and serial CTs to assess for ventricular size or may require ventricular drain placement. A number of patients will go on to require permanent CSF diversion (VP shunt).
Siehe auch:
- Intrazerebrale Blutung
- Arteriovenöse Malformation
- Subarachnoidalblutung
- Aneurysma
- Ependymom
- Kavernom
- Einblutung in die Basalganglien
- Lobärblutung
- Verschlusshydrocephalus
- intraventrikuläre Neoplasien und Läsionen - Überblick
- Hirnblutung mit Ventrikeleinbruch
- intraventrikuläre Blutung bei Neugeborenen
- paediatric intraventricular haemorrhage
- Einblutung in den Plexus choroideus
- intraventrikuläre arteriovenöse Malformation
- hypertensive haemorrhage
- basal ganglia hypertensive haemorrhage
und weiter:
- intraventrikuläre Neoplasien und Läsionen
- Intrakranielle Blutung
- ruptured berry aneurysm
- emergency CT head (mnemonic)
- fetal intracranial haemorrhage
- plexus choroideus cyst blood
- moya moya with haemorrhage
- Metastasen des Plexus choroideus
- primäre intraventrikuläre Blutung
- germinal matrix related intraventricular hemorrhage of the premature infant
- Subarachnoidalblutung nach Schlangenbiss


 Assoziationen und Differentialdiagnosen zu intraventrikuläre Blutung:
Assoziationen und Differentialdiagnosen zu intraventrikuläre Blutung:









