CNS cryptococcosis











CNS cryptococcosis results from infection of the central nervous system with the yeast-like fungus Cryptococcus neoformans. It is the most common fungal infection and second most common opportunistic infection of the central nervous system.
For a general discussion of infection with this organism, please refer to the article cryptococcosis.
Epidemiology
The disease tends to be predominant in immunocompromised individuals such as those with AIDS. In immunocompetent patients, there is usually history of close contact with birds.
Clinical presentation
Patients with cerebral cryptococcosis usually present with signs and symptoms of meningitis/meningoencephalitis including headache, seizures, altered mental state, focal neurological defect, or blurred vision due to raised intracranial pressure .
Pathology
Central nervous system involvement with cryptococcosis typically results from haematogenous spread from the lungs (which is usually the primary site). In HIV/AIDS patients cryptococcal infection of the CNS usually occurs when the CD4+ count drops below 100 cells/µL. The disease can have either meningeal or parenchymal involvement with the former being the primary manifestation . With meningeal involvement, a grayish, mucinous exudate accumulates over the involved brain surface.
There are three dominant CNS forms to the disease depending on which part of the brain is affected:
- meninges: meningitis
- parenchyma: cryptococcomas
- perivascular spaces: gelatinous pseudocysts
Meningitis and cryptococcomas are seen in immunocompetent hosts usually and gelatinous pseudocysts are more common in patients with HIV/AIDS.
Radiographic features
The disease can have a variety of radiographic presentations and is influenced by the degree of immunocompromise and therapy. As a result, the literature describing features has evolved considerably in parallel to marked improvements in the management of HIV and the availability of HAART.
As a general rule, in patients who are profoundly immunocompromised (and therefore earlier literature), cryptococcosis demonstrates little enhancement. Instead, in patients who are on more effective therapy enhancement is more frequently encountered .
The range of appearances includes
- hydrocephalus
- dilated perivascular spaces coalescing into gelatinous pseudocysts
- leptomeningeal and pachymeningeal enhancement
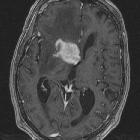
- cryptococcomas (or torulomas)
- miliary nodules
- choroid plexus (plexitis)
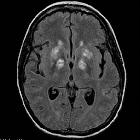
The most common pattern, particularly in profoundly immunocompromised patients is spread along the perivascular spaces, most commonly involving the basal ganglia but also the white matter of the cerebral hemispheres, the brainstem and cerebellum .
CT
CT findings can be often non-specific and with normal scans seen in a significant proportion of patients (reported up to ~40% ). Diffuse atrophy is usually the next most commonly described feature but may relate more to HIV dementia than cryptococcosis . Hydrocephalus and mass lesions may also each be present.
MRI
MRI is better at assessing dilated perivascular spaces, one of the most frequently described features on MRI, and basal ganglia pseudocysts. These findings are more common in immunocompromised patients. Signal characteristics can vary dependent on the form of infection.
Meningeal disease
- T1 C+ (Gd): can show leptomeningeal enhancement and pachymeningeal enhancement
- FLAIR C+ (post-contrast FLAIR): high T2 signal in subarachnoid space
Cryptococcomas
- T1: low signal
- T2/FLAIR: high signal
- T1 C+ (Gd): variable, ranging from no enhancement to peripheral nodular enhancement
- DWI/ADC: variable, may have both facilitated or restricted diffusion
Dilated perivascular spaces
Dilated perivascular space can coalesce into gelatinous pseudocysts that tend to give a "soap bubble" appearance.
- T1: low to intermediate (from mucin) signal
- T2: high signal
- FLAIR: variable signal ranging from full suppression to persistent high signal
- DWI/ADC
- variable; may have both facilitated or restricted diffusion
- maybe complicated by perforator infarct
Treatment and prognosis
Treatment is with appropriate antifungal (e.g. intravenous amphotericin B or fluconazole). If left untreated it is usually fatal.
Differential diagnosis
General imaging differential considerations include:
- other types of CNS infection
- CNS toxoplasmosis
- CNS tuberculosis
- pyogenic abscesses
- CNS lymphoma
Siehe auch:
- Tuberkulose des ZNS
- Abszess
- Neurotoxoplasmose
- primäres ZNS-Lymphom
- ZNS Lymphom
- sekundäres ZNS-Lymphom
- Kryptokokkose
- meningeale Kryptokokkose
und weiter:


 Assoziationen und Differentialdiagnosen zu zerebrale Kryptokokkose:
Assoziationen und Differentialdiagnosen zu zerebrale Kryptokokkose: