spinal cord metastases














Intramedullary spinal metastases are rare, occurring in ~1% of autopsied cancer patients, and are less common than leptomeningeal metastases.
Intramedullary lesions may result from:
- growth along the Virchow-Robin spaces
- haematogenous dissemination
- direct extension from leptomeninges
Epidemiology
Demographics of affected patients reflect those of the underlying primary malignancy but over all the mean age of presentation is 55 years . They represent 8.5% of central nervous system metastases and account for 5% of all intramedullary lesions.
Clinical presentation
Intramedullary spinal cord metastasis most commonly occurs in the setting of advanced disease and only rarely is the first presentation of malignancy .
In contrast to the long duration of symptoms that are typical of primary intramedullary spinal neoplasms, up to 75% of patients with a spinal cord metastasis have symptoms for less than one month before diagnosis .
The most common presenting symptom is motor weakness. Other common presenting features are pain, bowel or bladder dysfunction, paresthesia, or a rapid decline in neurological status in elderly patients .
Pathology
Lung cancer accounts for ~50% of cases . Other primary malignancies are: breast cancer, lymphoma, leukemia, malignant melanoma, renal cell cancer, colorectal cancer, cholangiocarcinoma , pancreatic neuroendocrine tumor , ovarian carcinoma , prostate carcinoma , gastric adenocarcinoma , uterine leiomyosarcoma (rare) , esophageal cancer , carcinoma of the uterine cervix , thyroid carcinoma , bladder carcinoma , salivary ductal carcinoma of the parotid gland .
One-third of patients have concomitant cerebral metastases and 25% have leptomeningeal metastases .
Radiographic features
The most commonly involved location is the cervical cord, followed by the thoracic cord and then the lumbar cord. Lesions are usually solitary and involve 2-3 vertebral body segments.
Plain radiograph
Usually normal.
CT
Hypervascular metastases may rarely be seen as enhancing intraspinal lesions.
CT myelography
Usually normal , although focal expansion or nodularity may be visible.
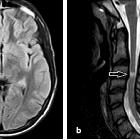
MRI
Lesions are usually well-defined and typically produce cord expansion over several segments. In contrast to primary intramedullary neoplasms, associated cysts are rare and some patterns of enhancement have been described as helpful in suggesting the diagnosis (see rim sign and flame sign below) . Typical MRI signal characteristics are:
- T1: hypointense
- T2
- hyperintense
- prominent edema commonly surrounds the tumor nodule
- T1 C+ (Gd):
- avid enhancement (seen in >80% of cases)
- peripheral thin region of increased enhancement (rim sign)
- ill-defined enhancement extending above and/or below the lesion (flame sign)
Treatment and prognosis
Management of intramedullary metastases generally consists of fractionated radiotherapy, which usually maintains but does not improve the pretreatment level of neurologic function. As with the treatment of brain metastases and epidural spinal cord compression, corticosteroids are used to diminish the effects of radiation-induced edema .
Intramedullary metastases are associated with a poor prognosis. Up to two-thirds of patients die within six months of diagnosis .
Differential diagnosis
General differential considerations include:
- other intramedullary spinal tumors, for example
- inflammatory lesions/transverse myelitis
- usually a longer length of cord involvement
- variable contrast enhancement
- rapidly progressive clinical course
- multiple sclerosis
- may not demonstrate enhancement
- less prominent cord expansion
- less prominent perilesional edema
- lesions are usually multiple
- syrinx
- central cystic lesion
- no contrast enhancement
See also
Siehe auch:
- Ependymom
- vertebrale Metastasen
- Transverse Myelitis
- Encephalomyelitis disseminata
- Syrinx
- Astrozytom
- Hämangioblastom
- intramedulläre spinale Tumoren
- spinale Meningeosis neoplastica
und weiter:


 Assoziationen und Differentialdiagnosen zu intramedullary metastases (spinal):
Assoziationen und Differentialdiagnosen zu intramedullary metastases (spinal):