ovarian neoplasms

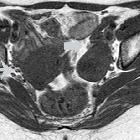
Krukenberg-Tumor
bei Magenkarzinom CT-morphologisch rechts dorsal des hyperperfundierten Uterus, histologisch war auch links eine Metastase des Ovars im Sinne eines Krukenberg-Tumors nachweisbar.

Epithelial
ovarian tumors • Serous cystadenoma of the ovary - Ganzer Fall bei Radiopaedia

Ovarian
tumors • Ovarian dysgerminoma - Ganzer Fall bei Radiopaedia

Ovarian
granulosa cell tumour: MR imaging findings. Axial contrast-enhanced T1-weighted image obtained with fat saturation shows intense and heterogeneous mass enhancement (arrow).

Ovary
mucinous cystoadenoma with components of a mucinous borderline tumor.
Ovarian
granulosa cell tumour: MR imaging findings. Transverse T1-weighted image shows an ovoid, well-delineated left adnexal mass lesion (arrow), mainly isointense to the normal uterus (long arrow).

Ovarian
tumors • Ovarian dermoid - Ganzer Fall bei Radiopaedia

Epithelial
ovarian tumors • Mucinous ovarian cystadenoma - Ganzer Fall bei Radiopaedia

Ovarian
tumors • Ovarian cancer with peritoneal carcinomatosis - Ganzer Fall bei Radiopaedia

Teratoma •
Ruptured ovarian teratoma - Ganzer Fall bei Radiopaedia

Ovarian
tumors • Ovarian mucinous cystadenoma - Ganzer Fall bei Radiopaedia

Epithelial
ovarian tumors • Ovarian serous cystadenofibroma - Ganzer Fall bei Radiopaedia

Epithelial
ovarian tumors • Ovarian serous cystadenocarcinoma - Ganzer Fall bei Radiopaedia

Endometrioid
carcinoma of the ovary • Endometrioid adenocarcinoma - Ganzer Fall bei Radiopaedia

Ovarian
tumors • Ovarian fibroma - Ganzer Fall bei Radiopaedia

Ovarian
granulosa cell tumour: MR imaging findings. Transverse T2-weighted image depicts inhomogeneous left adnexal mass (arrow), with signal intensity mainly similar to that of normal myometrium (not shown on this image), and small hyperintense areas, corresponding to internal cysts on pathology.

Adulter
Granulosazelltumor des Ovars in der Computertomographie (sagittale Rekonstruktion) bei einer 78-jährigen. Sehr großer, zystischer, multiseptierter Tumor mit soliden Anteilen.

Ovarian
tumors • Ovarian dysgerminoma - Ganzer Fall bei Radiopaedia

Ovarian
tumors • Brenner tumor of ovary (gross pathology) - Ganzer Fall bei Radiopaedia

Ovarian
tumors • Ovarian mucinous cystadenoma (gross pathology) - Ganzer Fall bei Radiopaedia

Ovarian
tumors • Ovarian fibroma (gross pathology) - Ganzer Fall bei Radiopaedia

Ovarian
tumors • Sclerosing stromal tumor of the ovary - Ganzer Fall bei Radiopaedia

Krukenberg
tumor • Krukenberg tumor of ovary (gross pathology) - Ganzer Fall bei Radiopaedia
Ovarian tumors are relatively common and account for ~6% of female malignancies. This article focuses on the general classification of ovarian tumors. For specific features, refer to the subarticles.
Pathology
Subtypes
Primary ovarian tumors
Surface epithelial-stromal ovarian tumors (60-70%):
- ovarian serous tumors
- ovarian serous cystadenoma: ~60% of serous tumors
- ovarian borderline serous cystadenoma: ~15% of serous tumors
- ovarian serous cystadenocarcinoma: ~25% of serous tumors; commonest malignant ovarian tumor
- ovarian mucinous tumors: ~20% of all ovarian tumors
- ovarian mucinous cystadenoma: ~80% of mucinous tumors
- ovarian borderline mucinous cystadenoma: 10-15% of mucinous tumors
- ovarian mucinous cystadenocarcinoma: 5-10% of mucinous tumors
- ovarian endometrioid tumor: 8-15% of all ovarian tumors
- clear cell ovarian carcinoma: ~5% of ovarian cancer
- Brenner tumor: ~2.5% of ovarian epithelial neoplasms
- squamous cell carcinoma of the ovary
- ovarian cystadenofibroma* / ovarian adenofibroma: can be serous, mucinous, endometrioid, clear cell or mixed
- ovarian cystadenocarcinofibroma: extremely rare
- ovarian fibrosarcoma
- undifferentiated carcinoma of the ovary: ~4% of all ovarian tumors
* sometimes classified as a separate category rather than under epithelial
Germ cell ovarian tumors (~20%):
- ovarian teratoma: the commonest primary benign tumor of the ovary
- ovarian dysgerminoma
- ovarian yolk sac tumor: endodermal sinus tumor
- ovarian embryonal carcinoma
- ovarian choriocarcinoma: <1% of ovarian tumors
- pure primary ovarian choriocarcinoma: extremely rare
- malignant mixed germ cell tumor of the ovary
Sex cord / stromal ovarian tumors (8-10%):
- ovarian fibrothecoma: ~5% of ovarian tumors
- ovarian fibroma: ~4% of ovarian tumors
- ovarian thecoma: ~1% of ovarian tumors
- sclerosing stromal tumor of the ovary: rare
- ovarian Sertoli-Leydig cell tumor - ovarian androblastoma: ~0.5% of ovarian tumors
- granulosa cell tumor of ovary: commonest malignant sex cord tumor
- small cell carcinoma of the ovary
Mixed
These are uncommon:
Other
- ovarian lymphoma
- metastases to the ovary
- Krukenberg tumor
- other metastatic lesions to the ovary
Classification according to morphology
Predominantly cystic
- serous cystadenoma
- mucinous cystadenoma
- mature cystic teratoma
- serous cystadenocarcinoma
- mucinous cystadenocarcinoma
Predominantly solid
- Brenner tumor
- thecoma
- fibroma
- endometroid granulosa cell tumors
- dysgerminoma
- endodermal sinus tumor (yolk sac tumor)
- metastatic
Serological tests
- CA-125 levels: elevated in most ovarian malignancies (~80% in general); some mucinous and germ cell tumors may not secrete this marker
- AFP levels: elevated particularly with immature ovarian teratomas (~50% of cases) and ovarian yolk sac tumors
- β HCG: in a small number of dysgerminomas
- human epididymis protein 4 (HE4): elevated in malignant ovarian diseases, being helpful to complement the Ca-125 in premenopausal women
Risk factors
General risk factors include
- nulliparity
- early menopause
- gonadal dysgenesis
- family history: contributes to 24% of cases of epithelial ovarian cancer
- BRCA1/BRCA2 mutations: particularly for serous types
- Lynch syndrome-associated ovarian cancers most often have an endometrioid or serous type histology
- smoking: especially for mucinous adenocarcinoma
- previous history of breast, endometrial or colon cancer (Lynch II)
- certain ethnic groups
Protective factors
- oral contraceptives
- breastfeeding (this is controversial)
Risk assessment
Staging
The FIGO staging system is used for almost all of the ovarian cancers: see ovarian cancer staging.
Siehe auch:
- Teratom des Ovars
- ovarian mucinous cystadenoma
- ovarian thecoma
- Krukenberg-Tumor
- adulter Granulosazelltumor des Ovars
- ovarian cystadenofibroma
- Zystadenom des Ovars
- seröses Boderline-Zystadenom des Ovars
- seröses Zystadenom des Ovars
- ovarian fibrothecoma
- Fibrom des Ovars
- FIGO-Klassifikation
- clear cell ovarian carcinoma
- ovarian dysgerminoma
- ovarian mucinous cystadenocarcinoma
- Ovarialkarzinom Staging
- ovarian borderline mucinous cystadenoma
- epithelial ovarian tumours
- Struma ovarii Tumor
- unreifes Teratom des Ovars
- ovarian mucinous tumours
- zystische Ovarialtumoren
- ovarian carcinoid tumours
- Brenner-Tumor
- Granulosazelltumor des Ovars
- Metastasen des Ovars
- sex cord - stromal ovarian tumours
- undifferentiated carcinoma of the ovary
- reifes zystisches Teratom des Ovars
- ovarian carcinosarcoma
- primary ovarian lymphoma
- specialised teratomas of the ovary
- juveniler Granulosazelltumor des Ovars
- ovarian yolk sac tumour
- Plattenepithelkarzinom des Ovars
- ovarian serous tumours
- ovarian cystadenocarcinofibroma
- Sertoli-Leydig-Zell-Tumor des Ovars
- malignant mixed germ cell tumour of the ovary
- benigne Tumoren des Ovars
- seröses Zystadenokarzinom des Ovars
- vorwiegend solide Ovarialtumoren
- Dottersacktumor des Ovars
- sclerosing stromal tumour of the ovary
- Adenofibrom des Ovars
- Kollisionstumor des Ovars / der Ovarien
- maligne Tumoren des Ovars
- Keimzelltumor des Ovars
- Chorionkarzinom des Ovars
- reines primäres Chorionkarzinom des Ovars
- mucinous adenocarcinoma
- ovarian androblastoma
- ovarian lymphoma
- ovarian endometrioid tumour
- ovarian papilliferous cystadenocarcinoma
- ovarian tumors in children
und weiter:
- Kystom
- Corpus luteum
- Milzmetastasen
- cancer
- ultrasound appearances of liver metastases
- verkalkte Metastasen
- Hydrokolpos
- ovaries
- hereditary non-polyposis colorectal cancer
- metastases to the breast
- sonographic values in obstetrics and gynaecology
- CA 125 elevation
- miliary nodules in the exam
- Ovar
- endometrioid carcinoma of the ovary
- predominantly solid ovarian neoplasms
- Hydrometrokolpos
- mucinous cystadenocarcinoma of ovary
- pelvine Aktinomykose
- peritoneale Pseudozysten
- Tubenkarzinom
- gynäkologisch radiologisches Curriculum
- mesonephroid carcinoma of the ovary
- ovarian tumours associated with endomterial thickening
- specialised teratoma of the ovary
- malignant mixed Müllerian tumour of the ovary
- ovarian cancer with peritoneal carcinomatosis
- reifes zystisches Teratom
- peritoneal pseudocyst
- multilokuläres muzinöses Zystadenom des Ovars
- ovarian involvement in Burkitt lymphoma
- carcinosarcoma of ovary
- MRI appearance of an ovarian fibroma
- Ovarialfibrom
- Metastasen in der Cervix uteri
- Hämangiom des Ovars


 Assoziationen und Differentialdiagnosen zu Neoplasien des Ovars:
Assoziationen und Differentialdiagnosen zu Neoplasien des Ovars:






ovarian
borderline mucinous cystadenoma








