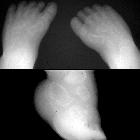
clubfoot















Congenital talipes equinovarus is considered the most common anomaly affecting the feet diagnosed on antenatal ultrasound.
Terminology
While some use talipes equinovarus and clubfoot synonymously, in certain publications, the term clubfoot is considered a more general descriptive term that describes three distinct abnormalities:
- talipes equinovarus (adduction of the forefoot, inversion of the heel and plantar flexion of the forefoot and ankle)
- talipes calcaneovalgus (dorsal flexion of the forefoot with the plantar surface facing laterally)
- metatarsus varus (inversion and adduction of the forefoot alone)
Epidemiology
It carries an estimated incidence of 0.5-5% of live births . Some reports suggest a male predilection with a male to female ratio of 2:1. The condition is bilateral in more than half of cases.
Pathology
The deformity involves both ankle and subtalar joints. The malalignment is fixed by joint, ligamentous and tendinous contractures.
There may be a familial predilection in ~15% of cases . If detected antenatally, a careful search for other associated anomalies is recommended.
Associations
There is an immense number (estimated at 200) of associations which include:
- chromosomal anomalies
- other syndromic conditions
- renal anomalies
- connective tissue disorders
- spinal anomalies
- skeletal dysplasias
Radiographic features
Plain radiograph
Assessment requires weight bearing DP and lateral radiographs. Where weight bearing is not possible, it should be simulated.
Talipes equinovarus consists of four elements :
- hindfoot equinus: lateral talocalcaneal angle less than 35º
- hindfoot varus: talocalcaneal angle less than 20º
- metatarsus adductus: adduction and varus deformity of the forefoot; talus to first metatarsal angle greater than 15º
- talonavicular subluxation: medial subluxation of the navicular on the talus
Ultrasound
Approximately 10-20% of individuals with prenatally diagnosed clubfoot may have a normal foot or positional foot deformity requiring minimal treatment. Conversely, 10-13% of prenatally diagnosed individuals with isolated clubfoot will have complex clubfoot postnatally, dependent on the presence of additional structural or neurodevelopmental abnormalities .
Sonographic features may vary depending on severity. Both the tibia and fibula may be in the same image as the medially deviated foot and the foot may additionally appear plantar flexed.
Treatment and prognosis
Many (at least 50%) require orthopedic intervention . The Ponseti method is a manipulative technique that corrects congenital clubfoot without invasive surgery. Therapeutic options range from casting and manipulation, through to surgical release. The most common surgical complication is overcorrection resulting in a "rockerbottom" flat foot deformity. Overall prognosis will often depend on other associated condition. Isolated condition may be treated successfully .
Siehe auch:
- Spina bifida
- caudal regression syndrome
- Ehlers-Danlos syndrome
- Meckel-Syndrom
- Marfan-Syndrom
- einseitige Nierenagenesie
- Trisomie 18
- Diastrophische Dysplasie
- Skelettdysplasie
- Roberts-Syndrom
- prune belly syndrome
- Diastematomyelie
- chromosomale Anomalien
- Freeman-Sheldon-Syndrom
- Talus verticalis
- Wolf-Hirschhorn-Syndrom
- De-Grouchy-Syndrom Typ 2
- rockerbottom
und weiter:
- cyllosoma
- Arthrogryposis multiplex congenita
- caudal dysplasia sequence
- Potter-Sequenz
- Myeloschisis
- Thalidomid-Embryopathie
- Larsen-Syndrom
- dysencephalia spanchnocystica
- kongenitale Kniegelenksluxation
- Salonen-Herva-Norio syndrome
- hydrolethalus
- Spondyloepimetaphysäre Dysplasie Typ Strudwick
- amyoplasia congenita
- angeborene Fußfehlbildungen
- kongenitaler Hydrozephalus


 Assoziationen und Differentialdiagnosen zu Klumpfuß:
Assoziationen und Differentialdiagnosen zu Klumpfuß:











