intraventricular neoplasms and lesions

Plexuspapillom
im vierten Ventrikel: Oben axial T2 , DWI, T1 nativ und FLAIR. Unten T2 sagittal und T1 KM sagittal, axial und coronar.




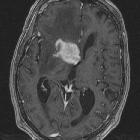
This 36
year-old male patient presented with a headache. This axial FLAIR (fluid-attenuated inversion recovery) MR image shows a right ventricular mixed solid/cystic mass limited by the septum pellucidum and ventricular walls. The solid portions of the tumour showed heterogeneous enhancement on post-gadolinium sequences. Based on these imaging characteristics a provisional diagnosis of central neurocytoma was made. The tumour was resected the next day - histology and immunocytochemistry confirmed the diagnosis.

Transcortical
approaches to large intraventricular tumors: a prospective case series of 20 patients. A large intraventricular central neurocytoma in a 25-year-old male patient, who presented with headaches and blurring of vision. a–c The preoperative axial, coronal, and sagittal contrast-enhanced brain MRI study. d–f The postoperative axial, coronal, and sagittal contrast-enhanced brain MRI study. Near-total excision of the tumor was achieved following a right frontal trans-cortical approach through the right middle frontal gyrus, leaving a small septal residue (white arrow)

Choroid
plexus metastases • Intraventricular metastasis from renal cell carcinoma - Ganzer Fall bei Radiopaedia

Ganglioglioma
• Intraventricular ganglioglioma - Ganzer Fall bei Radiopaedia

Primary CNS
lymphoma • Primary CNS lymphoma - intraventricular - Ganzer Fall bei Radiopaedia

Central
neurocytoma • Central neurocytoma - Ganzer Fall bei Radiopaedia

Subependymoma
• Subependymoma - lateral ventricle - Ganzer Fall bei Radiopaedia

Isolated
third ventricle glioblastoma. A multi-cystic heterogeneously enhanced mass is observed in the third ventricle on T1-weighted brain MR (a–c). Temporal horns are dilated despite previous V-P shunt surgery (d)

Intraventricular
neuroepithelial tumors: surgical outcome, technical considerations and review of literature. A 27-year-old female patient presented with slight headache and intermitting vertigo. Preoperative T1-weighted gadolinium enhanced MRI showing a heterogeneously enhancing intraventricular mass on the ground of the fourth ventricle consistent with an ependymoma (a,b). Postoperative T1-weighted gadolinium enhanced MRI showing complete removal of the tumor through a median suboccipital telovelar approach (c,d). Pathological findings confirmed WHO grade II ependymoma

Multiple
intraventricular metastases from lung adenocarcinoma with EGFR G719X mutation: a case report. MRI of brain during different periods of treatment a Contrast-enhanced MRI of brain showed heterogeneously enhancing lesions at the posterior horn of the right lateral ventricle and the IV ventricle, with upper ventricle hydrocephalus and edema of the surrounding parenchyma. T2FLAIR showed slightly higher signal of the masses. b Intraventricular lesions and surrounding area of edema observably shrunk with restored ventricular dilatation after 3-month treatment with afitinib. c Masses in the brain remain stable after 10-month treatment while lesions of lung progressed

Choroid
plexus carcinoma in an adolescent male: a case report. a T2 weighted image (T2WI) showing heterogeneous space occupying lesion (SOL) with necrotic areas with epicenter in left trigone of lateral ventricle infiltrating into adjacent white matter with surrounding vasogenic edema. (b) Postcontrast T1WI showing heterogeneous enhancement with multiple nonenhancing necrotic areas

Transcortical
approaches to large intraventricular tumors: a prospective case series of 20 patients. A large left sided intraventricular choroid plexus carcinoma in a 3-year-old female patient. a–c The preoperative axial, coronal, and sagittal contrast-enhanced brain MRI study. d–f The postoperative axial, coronal, and sagittal contrast-enhanced brain MRI study. Total excision of the tumor was achieved following a left posterior parietal trans-cortical approach

Transcortical
approaches to large intraventricular tumors: a prospective case series of 20 patients. A large intraventricular central neurocytoma in a 25-year-old male patient. a, b The preoperative axial and sagittal contrast-enhanced brain MRI study. c, d The postoperative axial and sagittal contrast-enhanced brain MRI study. Total excision of tumor was achieved following left frontal trans-cortical approach through the left middle frontal gyrus

Transcortical
approaches to large intraventricular tumors: a prospective case series of 20 patients. A large intraventricular central neurocytoma in a 33-year-old lady. a, b The preoperative axial and sagittal contrast-enhanced brain MRI. c, d The postoperative axial and sagittal contrast-enhanced brain MRI study. Total excision of tumor was achieved following left frontal trans-cortical approach through the left middle frontal gyrus

Transcortical
approaches to large intraventricular tumors: a prospective case series of 20 patients. Bilateral intraventricular sub-ependymal giant cell astrocytoma in an 8-year-old boy, who had generalized tonic-clonic convulsions. The patient had undergone an endoscopic biopsy and ventriculoperitoneal shunting, after which the seizures were controllable with medical treatment, and a decision of conservative management and serial follow-up imaging was taken. On 6-month follow-up, the seizures recurred and were difficult to control, and both tumors proved to have enlarged in size especially the right sided tumor. The right-sided tumor was surgically excised first through a right frontal trans-cortical approach, then the left-sided tumor was surgically excised in another session through a left frontal transcortical approach. a–c The initial axial, coronal, and sagittal contrast-enhanced brain MRI study. d–f Post-operative MRI following the first surgical session after excision of the right sided tumor which had enlarged during a 6-month follow-up period. g–i The final postoperative axial, coronal, and sagittal contrast-enhanced brain MRI study, which demonstrates total excision of both tumors. No CSF diversion was needed in this patient

Subependymal
giant cell astrocytoma (SEGA): a case report and review of the literature. Computed tomography scan revealing a voluminous mass in the perilateral ventricle with similar attenuation to that of cortical gray matter (a), following administration of a contrast product, the mass showed marked enhancement (b)

Atypical
central neurocytoma with leptomeningeal dissemination: a case report. MRI brain (contrast) showed a large, fairly defined lobulated heterogeneously enhancing space occupying lesion with its epicenter in subependymal region of right lateral ventricular body, showing gross extensions into the intraventricular space, thalamus, body of corpus callosum, and leftward displacement of septum pellucidum, with mild ventricular dilatation. There was a small eccentric non-enhancing cystic necrotic focus. A small focus, hypointense on T1 and hyperintense on T2 and FLAIR sequences with restricted diffusion on diffusion-weighted imaging (DWI) and heterogeneous post-contrast enhancement was seen involving left thalamus. No leptomeningeal enhancement was seen. a Axial T1 contrast sequence. b–d Axial, coronal, and sagittal T2 FLAIR sequences of the brain showing the tumor extensions

Intraventricular
neoplasms and lesions • Intraventricular neurocysticercosis - Ganzer Fall bei Radiopaedia

Choroid
plexus carcinoma: a rare cause of hydrocephalus. On contrast enhanced T1-weighted image, the choroid plexus carcinoma enhances vividly (arrows).

Choroid
plexus carcinoma: a rare cause of hydrocephalus. On T2-weighted image, the lesion is slightly heterogenous and hyperintense compared to white matter. Adjacent white matter shows vasogenic oedema that is considered to occur due to invasion of choroid plexus carcinoma (arrows).

Tuberöse
Sklerose in der MRT: Subependymales Knötchen im Seitenventrikel in der Nähe des Foramen Monroi mit deutlicher Kontrastmittelaufnahme. Die Entwicklung eines Riesenzelltumors kann nur im Verlauf (Größenzunahme oder Änderung der Kontrastmittelaufnahme) vermutet werden.

Tuberöse
Sklerose in der MRT: Hamartome (Tubera) subkortikal und subependymale Knötchen. T2 axial
This image
is part of a series which can be scrolled interactively with the mousewheel or mouse dragging. This is done by using Template:Imagestack. The series is found in the category Medulloblastoma - MRI - case 001. Medulloblastom in der MRT

This image
is part of a series which can be scrolled interactively with the mousewheel or mouse dragging. This is done by using Template:Imagestack. The series is found in the category Medulloblastoma - MRI - case 001. Medulloblastom in der MRT

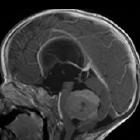
Zufallsbefund
einer Kolloidzyste am Foramen Monroi. Links axiale native Computertomographie, rechts coronare ebenfalls native MRT. Der Befund wurde nicht histologisch gesichert, ist aber typisch.

Intraventricular
neuroepithelial tumors: surgical outcome, technical considerations and review of literature. A 44-year-old female patient presented with aggravating headache, vertigo, gait disturbance and concentration disorder in sense of hydrocephalic symptoms for 3–4 months. a, b Preoperative T1-weighted gadolinium enhanced MRI showing a low to intermediate heterogeneously enhancing intraventricular mass in the third ventricle with consecutive secondary hydrocephalus. c, d Postoperative T1-weighted gadolinium enhanced MRI showing complete removal of the tumor through a left frontal precoronary transventricular keyhole approach. Pathological findings confirmed WHO grade I subependymoma

Intraventricular
neoplasms and lesions • Intraventricular meningioma - third ventricle - Ganzer Fall bei Radiopaedia

Intraventricular
neoplasms and lesions • Subependymal giant cell astrocytoma - tuberous sclerosis - Ganzer Fall bei Radiopaedia

Intraventricular
neoplasms and lesions • Colloid cyst - Ganzer Fall bei Radiopaedia

Intraventricular
neoplasms and lesions • Glioblastoma NOS (extending into ventricle) - Ganzer Fall bei Radiopaedia

Intraventricular
neoplasms and lesions • Cerebral intraventricular lung metastases - Ganzer Fall bei Radiopaedia

Choroid
plexus metastases • Choroid plexus metastasis - from renal cell carcinoma - Ganzer Fall bei Radiopaedia
Intraventricular neoplasms are rare and arise from periventricular structures such as the walls of the ventricular system, the septum pellucidum and the choroid plexus. Many tumor types arise from or can bulge into the ventricular system, although there are certain lesions that are relatively restricted to ventricles. A number of factors assist in defining the differential diagnosis, both radiological and clinical, including where the lesion is positioned within the ventricle as well as age and any associated conditions .
Neoplasms of the ventricular wall and septum pellucidum
Neoplasms of the choroid plexus
See: choroid plexus tumors.
Others
- intraventricular meningioma
- intraventricular metastasis
- oligodendroglioma
- pilocytic astrocytoma
- glioblastoma
- intraventricular CNS lymphoma
- medulloblastoma
- primitive neuroectodermal tumor
- sarcoma
- intraventricular teratoma
- chordoid glioma of the third ventricle
- rosette-forming glioneuronal tumors
Non-neoplastic lesions
See also
Siehe auch:
- Xanthogranulome des Plexus choroideus
- Pilozytisches Astrozytom
- Glioblastoma multiforme
- Tuberöse Sklerose
- Cavum septi pellucidi et vergae
- Oligodendrogliom
- Ependymom
- Neurozystizerkose
- intraventrikuläre Blutung
- Medulloblastom
- Kraniopharyngeom
- Hämangioblastom
- Tumoren der Pinealisregion
- primäres ZNS-Lymphom
- Plexuspapillom
- Kolloidzyste
- Karzinom des Plexus choroideus
- intraventrikuläres Meningeom
- Kolloidzyste des dritten Ventrikels
- intraventrikuläre Neoplasien und Läsionen - Überblick
- intraventrikuläres Neurozytom
- Subependymom
- subependymales Riesenzellastrozytom
- intraventrikuläre Arachnoidalzyste
- intraventrikuläre Arachnoidalzyste
- Tumoren des Plexus choroideus
- intraventrikuläre Kolloidzyste
- Primitiver neuroektodermaler Tumor des ZNS
- atypischer teratoider rhabdoider Tumor
- Tumoren des vierten Ventrikels
- intraventricular B cell lymphoma
- Metastasen des Plexus choroideus
- Trigonum Syndrom (Seitenventrikel)
- intraventrikuläre Metastasen
- intraventrikuläres Glioblastom
- intraventrikuläre arteriovenöse Malformation
- primitive neuroectodermal tumour
und weiter:


 Assoziationen und Differentialdiagnosen zu intraventrikuläre Neoplasien und Läsionen:
Assoziationen und Differentialdiagnosen zu intraventrikuläre Neoplasien und Läsionen: