metastases to the lungs



































Pulmonary metastases are common and the result of metastatic spread from a variety of primary tumors via blood or lymphatics.
This article describes haematogenous pulmonary metastases with lymphangitis carcinomatosis discussed separately.
Epidemiology
The epidemiology will match that of the underlying malignancy (see below), but as malignancies increase in incidence with increasing age, so does the presence of pulmonary metastases.
Clinical presentation
Pulmonary metastases are usually asymptomatic, with constitutional symptoms relating to disseminated metastatic disease and those attributable to the primary tumor dominating . Hemoptysis and pneumothorax are sometimes the presenting symptoms.
Pathology
Tumor cells reach the lungs via the pulmonary circulation, where they lodge in small distal vessels.
The most common primaries to result in pulmonary metastases in adults include :
- breast carcinoma
- colorectal carcinoma
- renal cell carcinoma
- uterine leiomyosarcoma
- head and neck squamous cell carcinoma
In the pediatric population, the most common primaries for pulmonary metastases are:
Alternatively, primaries which most frequently metastasize to lungs (although are much less common) include :
- choriocarcinoma
- Ewing sarcoma
- malignant melanoma
- osteosarcoma
- testicular tumors
- thyroid carcinoma
- pancreatic cancer
Primaries that metastasize as endobronchial deposits can include:
Radiographic features
Pulmonary metastases typically appear as peripheral, rounded nodules of variable size, scattered throughout both lungs . Atypical features include consolidation, cavitation, calcification, hemorrhage, and secondary pneumothorax.
Plain radiograph
Plain films are insensitive, although frequently able to make the diagnosis, as often pulmonary metastases are large and numerous.
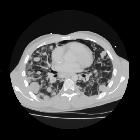
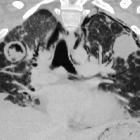
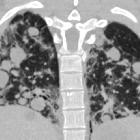
CT
CT is excellent at visualizing pulmonary nodules. Typically, metastases appear of soft tissue attenuation, well circumscribed, rounded lesions, more often in the periphery of the lung. They are usually of variable size, a feature which is of some use in distinguishing them from a granuloma .
A prominent pulmonary vessel has frequently been noted heading into a metastasis. This has been termed the feeding vessel sign . It is unclear whether this is a true finding or the result of older scanners with thicker slices resulting in volume averaging . However, a number of atypical features are commonly encountered.
Some tumors have a predilection for innumerable small metastases (miliary pattern):
Conversely, a pulmonary metastasis may be single. This is most frequently seen in colorectal carcinoma. Other primaries which often present with solitary metastases include :
- malignant melanoma
- skeletal sarcoma
- testicular carcinoma
- adenocarcinomas in general
Adenocarcinoma metastases, rather than displace or destroy adjacent lung parenchyma, may grow in a lepidic fashion (spread along alveolar walls) resulting in pneumonia-like consolidation. Air bronchograms may also be visible .
Cavitation is present in ~4% of cases . The most common primary is squamous cell carcinoma, most often from the head and neck or from the lung. Other primaries include adenocarcinomas, and sarcomas .
Calcification, although uncommon and more frequently a feature of benign etiology (e.g. granuloma or hamartoma) is also seen with metastases, particularly those from papillary thyroid carcinoma and adenocarcinomas. Treated metastases, osteosarcomas and chondrosarcomas may also contain calcified densities .
A halo of ground-glass opacity representing hemorrhage can be seen, particularly surrounding hemorrhagic pulmonary metastases, such as choriocarcinoma and angiosarcoma.
MRI
Although not used routinely, MRI may be as sensitive in the detection of pulmonary metastases as CT.
Treatment and prognosis
In general presence of pulmonary metastases is an ominous finding, indicating poor prognosis. The specific prognosis will, however, depend on the primary tumor.
Complications
Tumors with prominent necrosis located near a pleural surface may result in a pneumothorax. Osteosarcoma is classically described as the pulmonary metastasis that results in pneumothorax. Another cause of pneumothoraces includes cystic or cavitary pulmonary metastases.
Differential diagnosis
The differential depends on the number of nodules/masses and their imaging characteristics.
- differential of multiple pulmonary nodules
- differential of a single pulmonary nodule
- differential of miliary pulmonary nodules
- differential of a cavitating lung mass
- differential of a pulmonary mass with calcification
- differential of a pulmonary mass with surrounding ground-glass halo
Siehe auch:
- solitärer pulmonaler Rundherd
- miliare Lungenherde
- kavernisierende Lungenmetastasen
- Lungenmetastasen Pankreaskarzinom
- zystische Lungenmetastasen
- pulmonale Metastasierung Blasenkarzinom
- hyperdense pulmonale Raumforderungen
- pulmonary metastases from hepatic hemangiosarcoma
- differential of a cavitating lung mass
und weiter:
- Pneumatozele
- Pancoast tumour
- Phrenikusparese
- Pierre-Marie-Bamberger-Krankheit
- Kavernöse Lungenläsionen
- Lungenabszess
- multiple zystische Lungenherde
- angioinvasive pulmonale Aspergillose
- Magenulkus
- pulmonary opacification
- Interstitielle Lungenerkrankung
- interstitial pneumonia
- Rundpneumonie
- miliary nodules in the exam
- Organmetastasen
- Lungenmetastasen Wilmstumor
- Kleinzelliges Lungenkarzinom
- Lungentumor
- Thorax Onlinekurs
- benign metastasising leiomyoma
- acute airspace opacification with lymphadenopathy
- pulmonary manifestations of lymphomatoid granulomatosis
- Halozeichen Lunge
- Lungenmetastasen kolorektales Karzinom
- Lungenmetastasen bei Osteosarkom
- pulmonales Granulom
- lung metastases from hemangiopericytoma
- pulmonary metastases from hemangiosarcoma
- Lungenmetastasen bei Zervixkarzinom
- Metastasen Röntgenthorax
- multiple Lungenherde
- Lungenmetastasen bei Mammakarzinom
- Lungenmetastasen bei Magenkarzinom
- Radiofrequenzablation (RFA) bei pulmonalen Metastasen
- Lungenmetastasen bei Leiomyosarkom


 Assoziationen und Differentialdiagnosen zu Lungenmetastasen:
Assoziationen und Differentialdiagnosen zu Lungenmetastasen:


