Milzinfarkt


























Splenic infarction is a result of ischemia to the spleen, and in many cases requires no treatment. However, identification of the cause of infarction is essential.
Epidemiology
Splenic infarcts can occur due to a number of processes, involving either arterial supply, the spleen itself or the venous drainage. As such there is no one affected demographic; rather the demographics will vary with the underlying cause.
Clinical presentation
Patients with a splenic infarction may present with left upper quadrant pain. Some may have constitutional symptoms such as fevers and chills while others may even have diffuse abdominal pain. Due to the location of the spleen, tucked under the left hemidiaphragm, referred pain to the left shoulder is also a feature .
It should be noted that ~40% (range 30-50%) of patients with splenic infarction are asymptomatic .
Pathology
Etiology
The majority of patients with splenic infarcts have one of the following two etiologies:
- hematologic disorders
- more common in younger patients
- e.g. sickle cell disease
- hypercoagulable states
- embolic events
- more common in older patients
- e.g. infective endocarditis , marantic endocarditis
Other etiological factors include :
- splenic vascular disease
- splenic arterial aneurysms
- variant anatomy, e.g. wandering spleen, which may undergo splenic torsion
- collagen vascular disease
- pancreatitis
- non-hematologic malignancies
- blunt trauma: a segmental splenic infarct can occur as a rare complication
- splenic artery compression, e.g. by pancreatic tumor
- splenic embolization
- leukemia (CML most common)
Radiographic features
The appearance of splenic infarction depends on the timing of imaging and the size of the infarct. Although once the infarct has become established, both ultrasound and CT are sensitive to the diagnosis, in the hyperacute setting CT with contrast is the modality of choice if the diagnosis is suspected .
Morphologically the typical infarct is of a pyramidal wedge of affected splenic tissue with the apex pointing towards the hilum, and the base on the splenic capsule.
As the infarct matures, the wedge of infarcted tissue can undergo one of three processes which will dictate imaging features:
Ultrasound
Typically infarcts are hypoechoic compared to the rest of the spleen, although acutely they can be isoechoic and hard to identify. Sonographic features of acute splenic infarcts regarding shape can vary and include :
- wedge-shaped (classic)
- round
- irregularly
- smooth (uncommon)
During contrast-enhanced ultrasound, the infarcted area remains hypointense throughout all phases of the study .
As the infarct matures, if it undergoes contraction and scarring it will appear as a hyperechoic region with retraction of the capsule . If liquefaction occurs, the area may be rounded and anechoic (splenic pseudocyst).
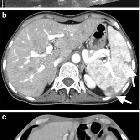
CT
CT is often considered the imaging investigation of choice, ideally performed during the portal venous phase, to avoid confusing heterogeneous enhancement normally seen during arterial phase. Imaging features may vary with the stage of the infarct.
In the hyperacute phase, CT may show areas of mottled increased attenuation, representing areas of a hemorrhagic infarction.
There are various classical and non-classical patterns of established splenic infarcts on CT, which include :
- peripheral, wedge-shaped hypoenhancing region: typical
- multiple infarcts appear as hypodense non-enhancing lesions, with normal intervening enhancing splenic tissue.
- global splenic infarction, entire spleen is hypoenhancing, e.g. in splenic torsion
- infarction of a splenunculus
In the chronic phase, infarcts may disappear completely, but more commonly, they may reveal progressive volume loss caused by fibrotic contraction of the infarct, with hypertrophy of the surrounding normal spleen . Alternatively, if the infarct liquefies, a cystic lesion may be left with fluid density centrally .
Treatment and prognosis
Initial management usually consists of hydration, analgesics, and frequent monitoring, with the resolution of symptoms in 7-14 days. Splenectomy was performed for persistent symptoms or complications.
Complications
Some complications are encountered, more frequently in patients with an embolic etiology. These include:
- formation of a splenic pseudocyst(s)
- infected splenic infarction leading to the formation of a splenic abscess
- splenic hemorrhage
- splenic rupture
Differential diagnosis
Often, when imaging appearances are typical, there is little differential diagnosis. When less typical, or when imaging is suboptimal, alternative diagnoses should be entertained, including :
- normal inhomogeneous splenic enhancement (zebra or psychedelic spleen): seen during arterial phase CT
- lymphoma
- usually rounded rather than wedge-shaped
- usually associated with splenomegaly and lymph node enlargement
- lymphoma may cause secondary splenic infarction potentially muddying the waters
- splenic abscess
- either primary or superimposed infection on a liquefied infarct
- splenic laceration
- history of trauma
- surrounding hematoma
- note: splenic rupture can complicate infarction
See also
Siehe auch:
- Splenomegalie
- Autosplenektomie
- Tigermilz
- fokale Milzläsionen und Anomalien
- septische Embolie Milz
- Lymphadenopathie
- Thrombose der Vena lienalis
- Thrombose der Arteria splenica
- Milztorsion
und weiter:


 Assoziationen und Differentialdiagnosen zu Milzinfarkt:
Assoziationen und Differentialdiagnosen zu Milzinfarkt:




