AKZ












































Aneurysmal bone cysts (ABC) are benign expansile tumor-like bone lesions of uncertain etiology, composed of numerous blood-filled channels, and mostly diagnosed in children and adolescents.
Epidemiology
Aneurysmal bone cysts are primarily seen in children and adolescents, with 80% occurring in patients less than 20 years of age .
Clinical presentation
Patients may present with pain, which may be of insidious onset or abrupt due to pathological fracture, with a palpable lump or with restricted movement.
Pathology
Aneurysmal bone cysts consist of blood-filled spaces of variable size that are separated by connective tissue containing trabeculae of bone or osteoid tissue and osteoclast giant cells. They are not lined by endothelium. A fine needle aspiration cytology is usually nondiagnostic, often dominated by fresh blood .
Although often primary, up to a third of aneurysmal bone cysts are secondary to an underlying lesion (e.g. fibrous dysplasia, osteosarcoma, giant cell tumor , chondromyxoid fibroma , non-ossifying fibroma , chondroblastoma ).
A variant of aneurysmal bone cysts is the giant cell reparative granuloma which is usually seen in the tubular bones of the hands and feet as well as in the craniofacial skeleton. Occasionally they are also seen in appendicular long bones where they are known as solid aneurysmal bone cysts. Histologically these two entities are identical .
Location
They are typically eccentrically located in the metaphysis of long bones, adjacent to an unfused growth plate. Although they have been described in most bones, the most common locations are :
- long bones: 50-60%, typically the metaphysis
- lower limb: 40%
- tibia and fibula: 24%, especially proximal tibia
- femur: 13%, especially proximally
- upper limb: 20%
- lower limb: 40%
- spine and sacrum: 20-30%
- especially posterior elements, with extension into the vertebral body in 40% of cases
- craniofacial: jaw, basisphenoid, and paranasal sinuses
- epiphysis, epiphyseal equivalent, or apophysis: rare but important
Radiographic features
Plain radiograph and CT
Radiographs demonstrate sharply defined, expansile osteolytic lesions, with thin sclerotic margins. CT will demonstrate these findings to a greater degree and is also better at assessing cortical breach and extension into soft tissues.
Additionally, CT can demonstrate fluid-fluid levels, which are harder to appreciate than on MRI and require viewing with a narrow window width .
Nuclear medicine
Bone scan
Doughnut sign: increased uptake peripherally with a photopenic center.
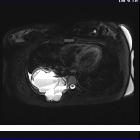
MRI
MRI is able to demonstrate the characteristic fluid-fluid levels exquisitely as well as identify the presence of a solid component suggesting that the aneurysmal bone cyst is secondary.
The cysts are of a variable signal, with a surrounding rim of low T1 and T2 signal. Focal areas of high T1 and T2 signal are also seen presumably representing areas of blood of variable age (see aging blood on MRI).
It is important to remember that the presence of fluid-fluid levels, although characteristic of aneurysmal bone cysts, is by no means unique to them, and is seen in other lesions as well, both benign and malignant (e.g. giant cell tumors (GCT), chondroblastoma, simple bone cysts and telangiectatic osteosarcomas).
- T1 (C+): septations may enhance
Angiography (DSA)
Aneurysmal bone cysts are poorly vascular .
Treatment and prognosis
Traditionally, these lesions have been treated operatively (curettage and bone grafting) with a recurrence rate of ~20% (range 11-31%). Percutaneous treatment with fibrosing agents has also been performed, either in isolation or as a precursor to surgical excision .
Spontaneous regression may occur, including following partial removal, but this is not the typical natural history .
Differential diagnosis
The differential diagnosis depends on the modality.
On plain radiography (and to a lesser degree CT), the diagnosis includes most of the lesions included in the mnemonic FEGNOMASHIC. Compared to the other lesions in this list, aneurysmal bone cysts are markedly expansile (hence, "aneurysmal") and have a thin cortical shell.
On MRI the differential is much shorter, especially when age, location and plain film appearance is taken into account. The main differential includes both lesions with intrinsic fluid-fluid levels (see fluid-fluid level containing bone lesions) and those from which an aneurysmal bone cyst may arise:
- chondroblastoma
- fibrous dysplasia
- giant cell tumor (GCT)
- osteosarcoma: especially telangiectatic osteosarcoma
Siehe auch:
- Fibröse Dysplasie
- Osteosarkom
- Lucent/lytic bone lesion - differential diagnosis (mnemonic)
- einfache (juvenile) Knochenzyste
- Chondroblastom
- Riesenzelltumor
- teleangiektatisches Osteosarkom
- aneurysmatische Knochenzyste der Patella
- fluid fluid level containing bone lesions
- Aneurysmatische Knochenzyste der Wirbelsäule
- Aneurysmatische Knochenzyste des Kalkaneus
- eingeblutete Knochenzysten
- solid variant of aneurysmal bone cyst
- secondary aneurysmal bone cyst
und weiter:
- Tumoren der Schädelkalotte
- Codman-Dreieck
- Periostreaktion
- nicht ossifizierendes Fibrom
- Ameloblastom
- vertebrale Metastasen
- Multiples Myelom
- dentigerous cyst
- spinal myxopapillary ependymoma
- Chondromyxoidfibrom
- clavicle abnormalities (paediatric)
- Türflügelzeichen
- radiologisches muskuloskelettales Curriculum
- single layer periosteal reaction
- spinales Ependymom
- Knochentumoren
- epiphysäre Knochentumoren
- Dens axis Zyste
- Tumoren der Thoraxwand
- WHO classification scheme for odontogenic tumours
- Riesenzelltumor des Knochens
- Knochenzyste
- osseous lesions preferentially involving the epiphysis
- liposklerosierender myxofibroider Tumor
- spinale Metastasen
- Morel Lavallée Läsion
- skeletal mass with fluid-fluid levels
- central giant cell granuloma
- spinales Ependymom des Filum terminale
- Läsionen des Sakrums
- Ostitis fibrosa cystica
- fibröser Kortikalisdefekt
- lytic bone lesion (mnemonic)
- Plasmozytom des Knochens solitär
- Osteoklastom
- Knochenläsionen der Epiphyse
- zystischer Knochentumor
- lytic rib lesion (mnemonic)
- paediatric clavicle abnormalities
- primary tumours of the spine
- WHO classification scheme for odontogenic tumours (1992)
- posterior vertebral body lesions (mnemonic)
- Läsionen der Mandibula
- benigne zystische oder zystoide Knochentumoren
- Riesenzelltumor des Beckenknochens
- hämophiler Pseudotumor
- Flüssigkeit-Flüssigkeitsspiegel
- Knochenläsionen der Metaphyse
- cysts humerus
- giant cell reparative cyst
- Aneurysmatische Knochenzyste des Os temporale
- mesenchymales Hamartom der Brustwand
- Aneurysmatische Knochenzyste der Orbita
- Aneurysmatische Knochenzyste des Beckens
- aneurysmatische Knochenzyste der Mandibula
- Aneurysmatische Knochenzyste des Femurs
- Aneurysmatische Knochenzyste und Fibröse Dysplasie
- Osteoblastom mit Aneurysmatischer Knochenzyste
- Aneurysmatische Knochenzyste der Tibia
- distribution of aneurysmal bone cysts (ABC)
- aneurysmal bone cyst - radius


 Assoziationen und Differentialdiagnosen zu Aneurysmatische Knochenzyste:
Assoziationen und Differentialdiagnosen zu Aneurysmatische Knochenzyste:









