moyamoya disease





















Moyamoya disease is an idiopathic, non-inflammatory, non-atherosclerotic progressive vasculo-occlusive disease involving the terminal supraclinoid internal carotid arteries and circle of Willis.
Terminology
The term moyamoya disease should be reserved for an idiopathic, sometimes familial, condition, which leads to characteristic intracranial vascular changes.
Numerous entities have been described which mimic the appearance, in which case the term moyamoya syndrome (or phenomenon or pattern) is used, which then can be further broadly divided into atherosclerotic causes and vasculitic/inflammatory causes .
This article concerns itself with moyamoya disease. For a list of conditions that can mimic moyamoya please refer to the article on moyamoya syndrome, or the differential diagnosis list at the end of the article.
Epidemiology
Moyamoya is a disease of children and young people, with a bi-modal age distribution :
The condition was initially described in Japanese patients, where it is still most common, in which 7-10% of cases are familial.
Clinical presentation
Presentation is to some degree age dependent. In children, hemispheric ischemic strokes are most pronounced, whereas in adults hemorrhage from the abnormal vessels is more common . Watershed infarcts are also very commonly identified.
Pathology
The underlying pathological and genetic basis for moyamoya disease is not well understood . Fibrocellular proliferation and thickening of the intima is the main process responsible for vascular stenosis and occlusion. The associated neo-vascularization may be a compensatory mechanism or part of the disease process itself, with the moyamoya vessels demonstrating various histopathological abnormalities including fibrin deposition, microaneurysm formation, among other abnormalities .
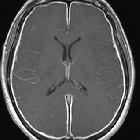
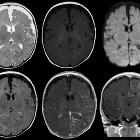
Radiographic features
General
Moyamoya disease affects the bilateral distal ICA and circle of Willis. Up to 18% of patients with moyamoya may present with unilateral angiography-documented disease.
Small abnormal net-like vessels proliferate giving the characteristic "puff of smoke" appearance on direct angiography. CTA and MRA are not always able to demonstrate this appearance on account of lower flow and spatial resolution.
Although classically described affecting the ICA, over 50% of patients also have involvement of the posterior cerebral arteries.
Generalized cerebral atrophy is a common finding.
Watershed infarcts are also commonly seen.
Collateral circulation forms from a number of sources:
- via the abnormal moyamoya vessels: lenticulostriate, thalamoperforating, leptomeningeal, and dural arteries appear as multiple tortuous flow voids on T1 and T2 weighted sequences
- pial collaterals from less affected vessels (especially PCA): forming the so-called ivy sign (high serpentine sulcal FLAIR signal intensity due to slow flow and also a high signal on T1 postcontrast-enhanced MRI)
- multiple foci of microbleeds and also prominent deep medullary veins "brush sign" on susceptibility sequences
- transdural branches of the middle meningeal and other dural branches
MRI
In addition to demonstrating the aforementioned arterial stenoses (best seen on MRA) or enlarged perforators (best seen on T2 weighted images), vessel wall imaging can also be helpful, particularly in distinguishing moyamoya disease from moyamoya syndrome from atherosclerotic or vasculitic/inflammatory causes .
Vessel wall imaging in moyamoya disease typically demonstrates :
- concentric luminal narrowing
- none or only minimal enhancement
- homogeneous T2 signal
- no outward remodeling (outer wall area of the stenotic segment greater than proximal normal segment; seen in atherosclerosis)
Staging
See: moyamoya staging (Suzuki)
Treatment and prognosis
Bypassing the occlusive segments is the aim of most surgical therapy and this can be accomplished by direct (i.e. direct artery-to-artery anastomosis) or indirect revascularization.
In adults, external carotid artery to middle cerebral artery (ECA-MCA) anastomoses can be performed as the vessels are larger. One of the surgical options is the superficial temporal artery to middle cerebral artery (STA-MCA) bypass.
A variety of indirect revascularization techniques have been developed, and are generally preferred in pediatric patients as their vessels are too small to allow direct anastomosis. These include :
- encephalomyosynangiosis (EMS)
- encephaloduroarteriosynangiosis (EDAS)
- encephaloduroarteriomyosynangiosis (EDAMS)
An alternative is to create multiple burrholes to allow formations of local collaterals .
History and etymology
The term moyamoya comes from a Japanese expression for something "hazy just like a puff of cigarette smoke drifting in the air" and was first described by Suzuki and Takaku in 1969 .
Differential diagnosis
A number of conditions can lead to imaging appearances that are very similar to moyamoya disease. For a full list, please refer to moyamoya syndrome:
- cranial radiotherapy
- atherosclerosis
- phakomatoses
- infection
- CNS vasculitides
- connective tissue disorders
- hematological disorders
Siehe auch:
- Tuberöse Sklerose
- Neurofibromatose Typ 1
- Sichelzellenanämie
- systemischer Lupus Erythematodes
- Phakomatosen
- Atherosklerose
- bakterielle Meningitis
- Moyamoya-Muster
- tuberkulöse Meningitis
- moyamoya staging (Susuki)
und weiter:


 Assoziationen und Differentialdiagnosen zu Moyamoya-Erkrankung:
Assoziationen und Differentialdiagnosen zu Moyamoya-Erkrankung: