lipomas












































Lipomas are benign tumors composed of mature adipocytes. They are the most common soft tissue tumor, seen in ~2% of the population.
Epidemiology
Patients typically present in adulthood (5-7 decades).
Associations
In some cases, multiple lipomas are associated with syndromes and other diseases, including:
- Bannayan-Zonana syndrome
- Cowden syndrome
- Fröhlich syndrome
- Proteus syndrome
- Dercum disease
- Madelung disease
- familial multiple lipomatosis
Clinical presentation
Typically lipomas are subcutaneous in location and present in adulthood as a soft painless mass in the trunk or proximal extremities. They are likely to have been present for many years and may change size with weight fluctuation.
Pathology
Benign lipomas are circumscribed soft masses, usually encapsulated, and composed almost entirely of fat. A small amount of non-adipose components are often present, representing fibrous septa, areas of fat necrosis, blood vessels, and interposed muscle fibers. Any non-adipose components must be carefully assessed to exclude a more aggressive component. Histology demonstrates mature adipocytes with no cellular atypia or pleomorphism .
A minority of lipomas are found in deeper locations and include intramuscular, intermuscular, intrathoracic, and retroperitoneal lipomas. These deep lipomatous masses should be assessed carefully, as they are more likely to be malignant. In fact, lesions in retroperitoneal location should be considered a well-differentiated liposarcoma until proven otherwise .
Intramuscular lipomas have nearly identical histology to superficial lipomas; however, intramuscular lesions tend to invade the adjacent musculature and commonly lack a capsule. Thus, these are sometimes known as infiltrating lipoma. In contradistinction, intermuscular lipomas do not exhibit local invasion and tend to be lobular or dumbbell-shaped, easily separated from adjacent soft tissues during surgical resection .
In 5-15% of patients, lipomas are multiple, and approximately a third of these will be familial .
Location
- central nervous system and spine
- head and neck
- thoracic
- abdominopelvic
- urogenital
- musculoskeletal
- vascular
- breast lipoma
Radiographic features
Superficial lipomas are typically well-circumscribed ovoid masses with homogeneous imaging characteristics of fat. A thin capsule, very thin septations (<2 mm), and scattered small areas of soft tissue density are common; however, avidly enhancing, thick/nodular septa or evidence of local invasion are suggestive of malignancy.
Plain radiograph
Large lipomas may be appreciated as a region of low density exerting mass effect. Calcification may be present in up to 11% of cases, although more commonly associated with well-differentiated liposarcoma .
Ultrasound
Lipomas appear as soft variably echogenic masses, commonly encountered on ultrasound. If encapsulated, the capsule may be difficult to identify on ultrasound .
According to a recent study, there is a wide range of appearance of biopsy-proven lipomas, with wide inter-reader variability (2004) :
- hyperechoic: 20-52%
- isoechoic: 28-60%
- hypoechoic: 20%
They also tend to display other ultrasound features, such as :
- no acoustic shadowing
- no or minimal color Doppler flow
Heterogeneous echotexture, more than minimal color Doppler flow, or large size is suspicious for liposarcoma.
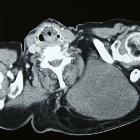
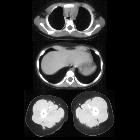
CT
Classic appearances are of a superficial circumscribed, low attenuation mass (typically approximately -65 to -120 HU) with minimal internal soft-tissue component. Again, areas of calcification may be present although are more frequently associated with well-differentiated liposarcoma .
Deeper or larger lesions may have scattered areas of internal soft-tissue density, often more apparent on CT versus MRI. These may represent areas of fat necrosis, fibrous tissue, blood vessels, or muscle fibers; these lesions cannot be confidently differentiated from liposarcoma by imaging.
Intramuscular lipomas may invade and interdigitate with the associated skeletal muscle, resulting in a characteristic striated appearance which may help distinguish from liposarcoma .
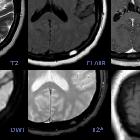
MRI
MRI is the modality of choice for imaging lipomas, not only to confirm the diagnosis, which is usually strongly suggested by ultrasound and CT but also to better assess for atypical features suggesting liposarcoma. Additionally, MRI is better able to demonstrate the surrounding anatomy.
As expected, lipomas follow subcutaneous fat signal on all sequences:
- T1
- high signal
- saturates on fat-saturated sequences
- no or minimal enhancement
- T2
- high signal on FSE T2
- saturates on fat-saturated sequences: persistent areas of high T2 signal are worrisome
When no suspicious features are present, the diagnosis of lipoma can be made with confidence with MRI being 100% specific . Similarly, if suspicious features are present, then the sensitivity of MRI is 100% , although specificity is lower, as some masses with atypical features will nonetheless be lipomas.
Treatment and prognosis
If all characteristics are those of a simple lipoma, and no local symptoms such as pain are present, then no treatment is generally required. However, resection for cosmesis is also a reasonable indication. If any concern exists, then biopsy or excision is required, with care taken about the approach in case the lesion is malignant. Recurrence rates of 4-5% are reported (most in deeper lesions) .
Differential diagnosis
In general, there is little differential for a classic soft tissue lipoma. The main differential is:
- liposarcoma
- low-grade tumors are difficult to differentiate from lipomas, and can have a relatively benign clinical course but suffer from high rate of recurrence
- normal adipose tissue
In certain locations, other fatty masses should be considered:
- retroperitoneum
- chest
Siehe auch:
- pleurale Lipome
- Angiomyolipom
- Myelolipom Nebenniere
- intraossäres Lipom
- Liposarkom
- Lipome des Gastrointestinaltraktes
- Thymuslipom
- parosteal lipoma
- kardiales Lipom
- Lipom der Speicheldrüsen
- lipomatöse Läsionen
und weiter:
- Lipom Sonographie
- tektales Lipom
- Gardner-Syndrom
- ektope Neurohypophyse
- WHO-Klassifikation der Tumoren des zentralen Nervensystems
- Lipoma arborescens
- Mukoidimpaktion
- Leiomyom Ösophagus
- subgaleal lipoma
- Steatocystoma multiplex
- pituitary region mass with intrinsic high T1 signal
- Lipoleiomyom des Uterus
- multiple endokrine Neoplasie Typ 1
- subarachnoid FLAIR hyperintensity
- WHO Klassifikation der Weichteiltumoren
- zerebellopontines Lipom (Lipom im Kleinhirnbrueckenwinkel)
- Hibernom
- Weichteillipom
- Lipom der Thoraxwand
- differential diagnosis for metatarsal region pain
- extraskeletal musculoskeletal tumors by compartment
- Galealipom
- Neurofibrom des Ösophagus
- extra skeletal musculoskeletal lesions by compartment
- Lipom versus Liposarkom
- parotid lipoma
- Weichteilschwellung Röntgen
- Bronchozele
- Lipom der Harnblase
- intraosseous lipoma of the parietal bone
- pelvine Lipomatose
- multiple hepatic lipomas
- Lipom mit Fettnekrose
- low grade liposarcomas (atypical lipomas) of the neck
- interkostales Lipom im Muskel
- bannayan zonana syndrome
- nasal encephalocoele
- paravertebral parosteal lipoma
- subcutaneous lipoma of the hand
- parosteal lipoma of the left zygomatic bone
- thoracic spine lipoma
- parosteal lipoma of the femur
- lipoma of thigh
- knee intra-articular lipoma
- Parapharyngealraum


 Assoziationen und Differentialdiagnosen zu Lipom:
Assoziationen und Differentialdiagnosen zu Lipom: