leptomeningeal carcinomatosis


























Leptomeningeal metastases, also known as carcinomatous meningitis, refers to the spread of malignant cells through the CSF space. These cells can originate from primary CNS tumors (e.g. drop metastases), as well as from distant tumors that have metastasized via haematogenous spread.
This article has a focus on subarachnoid space involvement. Refer to intradural extramedullary metastases for a discussion of leptomeningeal metastases in the spine. For other intracranial metastatic locations, please refer to the main article on intracranial metastases.
Epidemiology
The demographics follow those of the underlying malignancy.
Clinical presentation
Clinical presentation is varied, but most commonly includes a headache, spine or radicular limb pain or sensory abnormalities, nausea and vomiting, and focal neurological deficits . Meningism is only present in a minority of patients (13% ).
Pathology
The primary intracerebral malignancies that may cause metastases to the subarachnoid space are:
- glioblastoma (GBM) and anaplastic astrocytoma
- medulloblastoma
- sPNET
- ependymoma
- germinoma
- choroid plexus carcinoma
- pineoblastoma/pineocytoma
The vast majority of leptomeningeal metastases occur in the context of a widespread metastatic disease, likely by haematogenous spread. Over 50% of cases have concurrent brain (parenchymal) metastases . The most common primary sites are:
- breast cancer (particularly infiltrating lobular carcinoma)
- lung cancer
- melanoma
- gastrointestinal (gastric carcinoma , colorectal cancer )
- hematological: lymphoma/leukemia: may be called leptomeningeal lymphomatosis
Less common, but reported primary sites include:
- pancreatic carcinoma
- ovarian cancer
- renal cell cancer
- carcinoma of the uterine cervix
- adrenal cortical carcinoma
- esophageal cancer
- urinary bladder adenocarcinoma
- prostate cancer
- malignant pleural mesothelioma
- testicular cancer
- intradural malignant peripheral nerve sheath tumor (MPNST)
- anaplastic thyroid carcinoma
- transitional cell carcinoma of the bladder
- cholangiocarcinoma (extremely rare)
Radiographic features
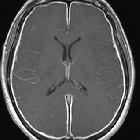
MRI
- T1: usually normal
- T1 C+ (Gd): leptomeningeal enhancement is the primary mode of diagnosis, often scattered over the brain in a 'sugar coated' manner
- T2: usually normal
- FLAIR
- abnormally elevated signal within sulci
- can be performed both non-contrast and post-contrast, but is slightly less specific if performed post-contrast
Treatment and prognosis
Leptomeningeal metastases have a poor prognosis with patients usually succumbing within a few months (median overall survival 2.4 months ). With treatment, that time may be extended up to 6-10 months . Treatment can consist of :
- intrathecal chemotherapy
- radiotherapy
Resection is usually inappropriate due to the presence of widespread metastases.
Differential diagnosis
- leptomeningeal inflammation: leptomeningitis
- slow flow in vessels
- propofol, high oxygen tension, and subarachnoid blood can all elevate sulcal FLAIR signal
Siehe auch:
- meningeale Kontrastmittelaufnahme
- Neurosarkoidose
- Liquorunterdrucksyndrom
- Meningitis
- spinale Meningeosis neoplastica
- bakterielle Meningitis
- Meningeosis leukaemica
- Tuberkulose der Wirbelsäule und des Spinalkanals
- tuberkulöse Meningitis
- Metastasen der Dura
- Erweiterung der Schädelnähte bei Meningeosis leukaemica
- leptomeningeale Abtropfmetastasen
- Meningeosis lymphomatosa
- spinale Meningeosis lymphomatosa
und weiter:
- Tuberkulose des ZNS
- leptomeningeale Kontrastmittelanreicherungen
- Knochenmetastasen des Schädels
- bilateral middle cerebellar peduncle lesions
- subarachnoid FLAIR hyperintensity
- diffuse leptomeningealer glioneuronaler Tumor (DLGT)
- meningeale Tumoren
- Tuberkulom des ZNS
- idiopathische hypertrophe Pachymeningitis
- Myelonkompression durch Metastasen
- Meningitis CCT
- meningeale Beteiligung bei Morbus Hodgkin
- Meningeosis LWS
- postiktale Veränderungen in der MRT
- dural metastases from prostatic carcinoma
- meningeale Metastasen
- Lymphom der Dura
- meningotheliale Hyperplasie


 Assoziationen und Differentialdiagnosen zu Meningeosis neoplastica:
Assoziationen und Differentialdiagnosen zu Meningeosis neoplastica: