juvenile pilocytic astrocytoma (JPA)
















































Pilocytic astrocytomas, also known as juvenile pilocytic astrocytomas, are low-grade, relatively well-defined astrocytomas that tend to occur in young patients. They are considered WHO grade I tumors in the current (2016) WHO classification of CNS tumors and correspondingly have a relatively good prognosis.
These tumors have a range of imaging appearances, with the majority presenting as a large cystic lesion with a brightly enhancing mural nodule. Calcification can be present in around one-fifth of cases.
The majority of pilocytic astrocytomas arise from the cerebellum. Optic pathway gliomas and spinal cord pilocytic astrocytomas are discussed separately.
The remainder of this article focuses on a general discussion of pilocytic astrocytomas, particularly those in the cerebellum.
Epidemiology
Pilocytic astrocytomas are tumors of young people, with 75% occurring in the first two decades of life, typically late in the first decade (9-10 years). There is no recognized gender predisposition.
Although only accounting for between 0.6-5.1% of all intracranial neoplasms (1.7-7% of all glial tumors) they are the most common primary brain tumor of childhood, accounting for 70-85% of all cerebellar astrocytomas and 15% of all pediatric brain tumors .
Associations
There is a strong association with neurofibromatosis type 1 (NF1). NF1 associated tumors have a tendency to affect the optic nerves and chiasm (see: optic pathway glioma). The association between NF1 and pilocytic astrocytomas is so strong that up to 20% of all patients with NF1 will develop these tumors, typically in early childhood. Conversely, approximately one-third of pilocytic astrocytomas involving the optic nerves have associated NF1.
Clinical presentation
Presentation depends on location. In the posterior fossa tumors, there is predominantly a mass effect with signs of raised intracranial pressure, especially when hydrocephalus is present. Bulbar symptoms or cerebellar symptoms may also be present.
Pathology
Location
By far the most common location is the cerebellum, with optic pathway being the next most common, particularly in patients with neurofibromatosis type 1. The distribution within the cerebellum varies with many tumors involving both the vermis and the cerebellar hemisphere.
In general, pilocytic astrocytomas typically arise from midline structures.
- cerebellum
- 60%
- optic pathway (optic nerve, optic chiasm, hypothalamus, optic radiation)
- 25-30%, particularly common in NF1
- see: optic pathway glioma
- other less common locations
- brainstem
- cerebral hemispheres: more frequent in adults
- cerebral ventricles
- velum interpositum
- spinal cord, see: spinal pilocytic astrocytoma
Microscopic appearance
The term pilocytic refers to the elongated hair-like projections from the neoplastic cells . The presence of eosinophilic Rosenthal fibers is a characteristic feature and hyalinization of blood vessels is also common. The histological features are however, fairly heterogeneous even within the one tumor, with some areas mimicking diffuse astrocytomas and even oligodendrogliomas .
Immunophenotype
Immunohistochemistry reflects astrocytic differentiation :
- GFAP: positive
- S100: positive
- OLIG2: positive
- IDH R132H mutation: negative
- p53 protein: negative or weak
Genetics
Pilocytic astrocytoma, as well as pleomorphic xanthoastrocytomas, frequently have BRAF alterations (present in ~70% of cases). Importantly they, along with other pediatric low-grade gliomas, lack IDH mutations and TP53 mutations .
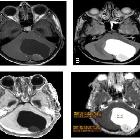
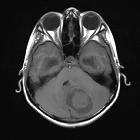
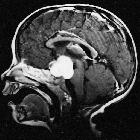
Radiographic features
General
Pilocytic astrocytomas range in appearance:
- large cystic component with a brightly enhancing mural nodule: 67%
- non-enhancing cyst wall: 21%
- enhancing cyst wall: 46%
- heterogeneous, mixed solid and multiple cysts and central necrosis: 16%
- completely solid: 17%
Enhancement is almost invariably present (~95%). Up to 20% may demonstrate some calcification. Hemorrhage is an uncommon complication.
MRI
- T1
- solid component: iso to hypointense compared to adjacent brain
- cystic component: ~fluid signal unless hemorrhage
- T1 C+
- vivid contrast enhancement
- the cyst wall enhances in ~50% cases
- T2
- solid component: hyperintense compared to adjacent brain
- cystic component: high signal
- T2*:
- signal loss if calcification or hemorrhage present
Treatment and prognosis
They are slow growing well-circumscribed tumors with an overall good prognosis following treatment (5-year and 10-year survival >95%) . Cystic tumors have even better prognosis while fibrillary variants tend to do worse.
Surgical resection, if complete, is usually curative. Some surgeons advocate that only the nodule need be resected to effect a cure, as the cyst walls are non-neoplastic, even if enhancing .
History and etymology
In 1931, Harvey Cushing was the first who described this tumor, based on his studies of 76 cases of cerebellar astrocytomas . Pilocytic means hair-like and is derived from the Latin word pilus for hair.
Differential diagnosis
General imaging differential considerations include:
- hemangioblastoma
- usually seen in adults. In children, usually associated with von Hippel-Lindau disease
- cyst wall usually does not enhance
- doesn't show calcifications
- smaller mural nodule with angiographic contrast blush
- medulloblastoma
- typically arise from the midline (especially vermis and roof of the fourth ventricle) rather than cerebellar hemisphere
- usually seen in younger patients (2-6 years of age)
- atypical teratoid/rhabdoid tumor
- larger heterogeneously enhancing mass
- ependymoma
- tends to fill the fourth ventricle and protrude out of the foramen of Luschka and foramina of Magendie
- large cystic component less common
- cerebellar abscess
- has a different clinical presentation
- no enhancing nodule
- ganglioglioma
- pleomorphic xanthoastrocytoma (PXA)
- ischemic stroke
- cerebellar hemorrhage
Siehe auch:
- Hirnabszess
- Tumoren der Hypophysenregion
- Ependymom
- Gangliogliom
- Medulloblastom
- Astrozytom
- Hämangioblastom
- Pleomorphes Xanthoastrozytom
- Kleinhirntumoren
- Morbus Hippel-Lindau
- spinales Pilozytisches Astrozytom
- atypischer teratoider rhabdoider Tumor
- Pilozytisches Astrozytom des Kleinhirns
- pilomyxoides Astrozytom
- zystisches Astrozytom
und weiter:
- Arachnoidalzyste
- Neurofibromatose Typ 1
- intraventrikuläre Neoplasien und Läsionen
- Pituitary MRI (an approach)
- WHO-Klassifikation der Tumoren des zentralen Nervensystems
- neuroradiologisches Curriculum
- Opticusgliom
- Dysembryoplastischer neuroepithelialer Tumor
- Tumoren der hinteren Schädelgrube
- Kolloidzyste des dritten Ventrikels
- intraventrikuläre Neoplasien und Läsionen - Überblick
- Hirntumoren
- Morbus Alexander
- diffuses Astrozytom
- posterior fossa astrocytoma
- focal brainstem glioma
- suprasellar / hypothalamic lesions
- mass involving the foramen of Monro or/and superior third ventricle
- teratoma suprasellar
- infratentorielles pilozytisches Astrozytom
- juveniles zerebelläres pilozytisches Astrozytom
- rosenthal fibres
- Pilozytisches Astrozytom des Nervus opticus
- differential diagnoses for temporal lobe tumours
- Grading Astrozytom


 Assoziationen und Differentialdiagnosen zu Pilozytisches Astrozytom:
Assoziationen und Differentialdiagnosen zu Pilozytisches Astrozytom:









