agenesis of the corpus callosum







































Dysgenesis of the corpus callosum may be complete (agenesis) or partial and represents an in utero developmental anomaly. It can be divided into:
- primary agenesis: the corpus callosum never forms
- secondary dysgenesis: the corpus callosum forms normally and is subsequently destroyed
Epidemiology
A true estimate of incidence is difficult to establish as many isolated cases are asymptomatic. It may be as uncommon as 1:20,000 according to autopsy series . It should be noted however that in pediatric neuroradiology practice it may be seen in as many as 1% of referrals, clearly representing a significant selection bias, attributable to a large number of symptomatic associated abnormalities.
There appears to be a male predilection (M:F ~2:1) . Maternal alcohol consumption during pregnancy has been recognized as another risk factor .
Associations
Associated anomalies can be frequent and broad which includes:
- aneuploidy syndrome
- non-aneuploidy syndrome
- other CNS associations: often multiple present
- Chiari II malformation (7%)
- Dandy-Walker spectrum (11%)
- grey matter heterotopia
- holoprosencephaly
- hydrocephalus (30%): particularly the trigones and posterior horns of lateral ventricles = colpocephaly
- interhemispheric cysts
- intracranial lipoma (10%)
- polymicrogyria
- porencephaly
- schizencephaly
- inborn errors of metabolism
- non-ketotic hyperglycemia
- pyruvate metabolism disorders
- congenital lactic acidosis (due to mitochondrial respiratory chain defects)
- mucopolysaccharidoses
- mucolipidoses
Clinical presentation
Isolated partial dysgenesis of the corpus callosum is often asymptomatic. The clinical picture in other cases is dictated by the associated abnormalities that are frequently found, especially in agenesis .
Children with agenesis may have dysmorphic facies, most commonly demonstrating hypertelorism .
Pathology
Agenesis is a result of an insult occurring at approximately 8-12 weeks gestation resulting in failure to form the corpus callosum. The white matter tracts which usually cross the midline, instead are oriented vertically, separating the lateral ventricles widely, in a racing car sign configuration. These bundles of white matter are known as Probst bundles.
The anterior commissure is usually present and often enlarged. The hippocampal formations are usually hypoplastic, with resultant dilatation of the temporal horns of the lateral ventricles.
Dysgenesis (which may be complete or partial) is a result of encephalomalacia secondary to toxic, ischemic or traumatic events .
Embryology
The development of the corpus callosum occurs between the 12 and 16-20 weeks of gestation . It begins with the genu and then continues posteriorly along the body to the splenium. The rostrum is the last part to be formed. In primary dysgenesis parts of the corpus callosum which form before the insult will be present whereas later parts will be absent. The presence of the rostrum essentially excludes primary agenesis.
One apparent exception to this rule is holoprosencephaly in which it is the anterior parts of the corpus callosum which are absent . This has been termed atypical callosal dysgenesis.
Myelination of the corpus callosum occurs in the opposite direction, from the splenium forwards.
Radiographic features
As with other structural anomalies, all modalities reflect the underlying morphology, with a greater lesser degree of sensitivity.
Antenatal ultrasound
- third ventricle
- dilated
- can be elevated or dorsally displaced
- may communicate with the interhemispheric cistern
- may project superiorly as a dorsal cyst
- choroid may be seen as an echogenic structure in the roof of the cyst
- lateral ventricles
- widely spaced parallel bodies (racing car sign)
- small frontal horns
- colpocephaly: which can give a "teardrop" configuration on axial scans
- septum pellucidum: absent
- interhemispheric fissures: widened
- gyri: may be seen in a "sunray appearance" on the sagittal plane
- color Doppler study may show an abnormal course of pericallosal arteries
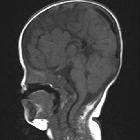
MRI
MRI is the modality of choice in evaluating both the corpus callosum and the frequently associated anomalies. Features include:
- ventricles
- run parallel rather than the normal "bow-tie" configuration giving a racing car appearance on axial imaging
- colpocephaly (dilatation of the trigones and occipital horns) gives a characteristic "Texas longhorn"/moose head/viking helmet appearance on coronal imaging
- dilated high-riding 3 ventricle appears to communicate with the interhemispheric cistern or project superiorly as a dorsal cyst
- cortex
- bundles of Probst
- radial gyri (absent cingulate gyrus)
- everted cingulate gyrus
- limbic system
- hypoplastic fornices
- hypoplastic hippocampi
Angiography
Angiography no longer has a role in diagnosis, however, if performed for other reasons may demonstrate an abnormal course of the anterior cerebral artery, passing directly posterosuperiorly with widely spaced pericallosal arteries, and absent pericallosal moustache. The azygos ACA is commonly present in most of the cases.
Treatment and prognosis
The overall prognosis can be highly variable depending on the presence of other associated anomalies.
Differential diagnosis
High-quality MRI essentially eliminates differentials due to the exquisite imaging of the corpus callosum.
In the setting of an antenatal ultrasound demonstrating an interhemispheric cyst then the following should be considered :
- cavum septum pellucidum
- cavum vergae
- cavum velum interpositum
- interhemispheric arachnoid cyst
The key to distinguishing these entities from a dilated third ventricle with dorsal cyst is identifying the choroid plexus, which demarcates the roof of the third ventricle .
Siehe auch:
- Arachnoidalzyste
- Falxlipom
- Balkenlipom
- Cavum septi pellucidi et vergae
- Cavum septi pellucidi
- Balkenatrophie
- Balkenmangel
- Cavum veli interpositi Zyste
- longitudinal callosal fascicle
und weiter:
- Tuberöse Sklerose
- tektales Lipom
- Pätau-Syndrom
- Gorlin-Goltz-Syndrom
- Balkenläsionen
- Hypertelorismus
- lemon sign
- Meckel-Syndrom
- Heterotopie der grauen Substanz
- azygote Arteria cerebri anterior
- Kolpozephalie
- bickers Adams Edwards syndrome
- Arthrogryposis multiplex congenita
- Aicardi-Goutières-Syndrom
- Coffin-Siris syndrome
- Kolobom
- enlarged fetal ventricles
- orbital hypertelorism
- Tumor im Corpus callosum
- Walker-Warburg-Syndrom
- fetal intra-cranial cystic lesions
- classification system for midline abnormalities of the brain and skull
- paediatric curriculum
- Fryns-Syndrom
- dysencephalia spanchnocystica
- Frontonasale Dysplasie
- probst bundles
- Salonen-Herva-Norio syndrome
- Wolf-Hirschhorn-Syndrom
- hydrolethalus
- Graham-Cox-Syndrom
- incomplete partition type 1 - cystic cochleovestibular malformation
- atypical callosal dysgenesis
- fetal arachnoid cyst
- Chiari-Malformation Typ 3
- racing car sign
- recurrent spontaneous hypothermia with hyperhidrosis syndrome
- median cleft syndrome
- MASA-Syndrom
- Wikingerhelm-Zeichen
- multiple sclerosis associated with complete corpus callosum agenesis
- pericallosal lipoma and callosal dysgenesis
- ribbon lipoma with corpus callosal dysgenesis
- tuber cinereum hamartoma with corpus callosal hypoplasia
- Elchkopf-Zeichen
- Balkenhypoplasie Leukodystrophie
- lipoma of dysgenetic corpus callosum


 Assoziationen und Differentialdiagnosen zu Dysgenesie des Corpus callosum:
Assoziationen und Differentialdiagnosen zu Dysgenesie des Corpus callosum:



